
Remember me
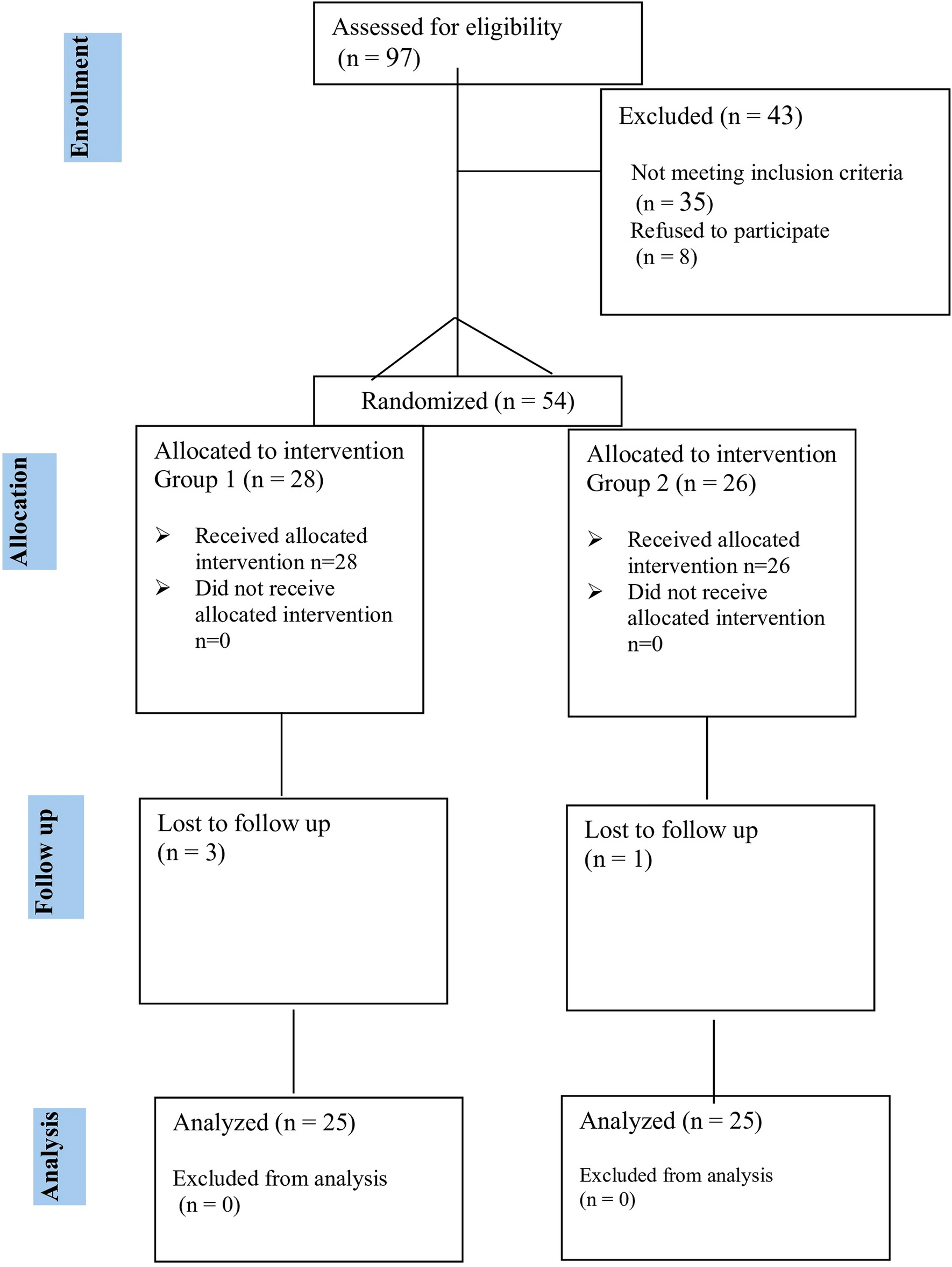
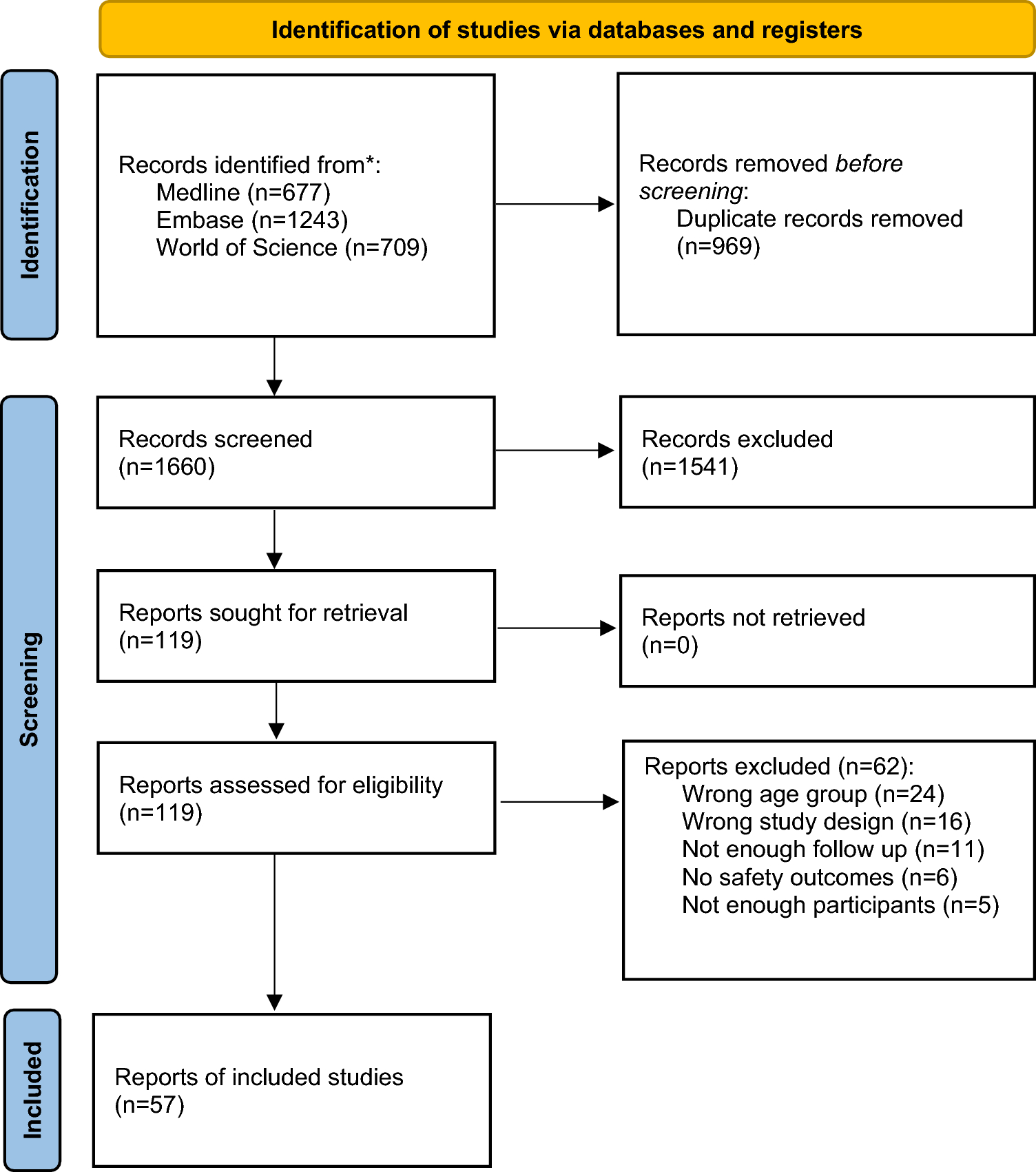
A total of 2629 records were identified on the initial search (1660 unique records after de-duplication); 119 full texts were sought for retrieval. All 119 were retrieved and assessed for eligibility. In total, 57 studies were included in the review. Figure 1 details the study selection process using the PRISMA 2020 flow diagram format [7]. Reasons for full text exclusion are documented in the excluded study table in the Supplementary Information.
Fig. 1
PRISMA flow diagram showing study selection process [7]
3.2 Study CharacteristicsIn total, 57 studies were included in the review, including a total of 3690 anti-IL-1-medication-exposed patients (excluding one study that did not report the total number of included patients [9]). Total duration of medication exposure has not been presented, as many studies did not include mean or total time on treatment. Extracted data and risk of bias assessments are detailed in the included study characteristics tables in the Supplementary Information.
Among the included studies were retrospective cohort studies (n = 31), registry based observational studies (n = 10), open label prospective studies (n = 5), randomised controlled trial (RCT) studies (n = 4), RCT long-term extension (LTE) studies (n = 4), prospective cohort studies (n = 2) and a post-marketing pharmacovigilance reporting system study (n = 1).
The smallest included studies were retrospective cohort studies of ten patients [10,11,12], while the largest was a retrospective cohort study including 335 anti-IL-1-medication-exposed patients [13]. There was also a large Food and Drug Administration Adverse Event Reporting System (FAERS) post-marketing pharmacovigilance study that reported 28,496 canakinumab-related adverse events but did not report the total number of included patients [9]. The median number of included patients per study was 43.
In total, 34 (59.6%) of the included studies had a female predominance, and 18 (31.6%) had a male predominance. The earliest report was published in 2009 [14], while the most recent was in 2025 [9]. Studies were based in Türkiye (n = 16), the USA (n = 5), France (n = 4), Germany (n = 4), the UK (n = 3), Israel (n = 2), Italy (n = 2), Japan (n = 2), China (n = 1), Czech Republic (n = 1), Netherlands (n = 1), Russia (n = 1) and Saudi Arabia (n = 1). A total of 14 were performed across multiple countries.
Disease cohorts included juvenile idiopathic arthritis (including SJIA) (24 studies, 2001 patients) and defined SAIDs including familial mediterranean fever (FMF) (11 studies, 338 patients), cryopyrin-associated periodic syndromes (CAPS) (7 studies, 135 patients) and mevalonate kinase deficiency (MKD) (1 study, 74 patients). In total, 14 studies included multiple conditions and/or undifferentiated SAIDs (14 studies, 1142 patients).
A total of 15 studies (1009 patients) reported on anakinra, 23 (1485 patients) on canakinumab, 2 (94 patients) on rilonacept and 17 (1102 patients) reported on multiple anti-IL-1 medications (Table 1).
Table 1 Included studies by medication and indicationSeveral studies were assessed as likely overlapping with regard to included patients. In total, two studies reported on the long-term effect of canakinumab in patients with SJIA from several trials (NCT00891046, NCT00889863 and NCT00886769) [15, 16]. In total, three studies reported on the multinational JIRcohorte registry [17,18,19], and four studies reported on the German BIKER registry [20,21,22,23]. A total of two studies reported results from the CLUSTER trial; one limited to canakinumab-treated patients with MKD [24] and the other to patients with colchicine-resistant FMF [25]. In total, two studies reported on results from a prospective open label study on anakinra in patients with severe CAPS (NCT00069329) [26, 27]; two studies described outcomes in anakinra-treated patients with SJIA in Italy and shared the same ethics committee reference number (364-16OCT2013) [28, 29].
3.3 Risk of Bias in StudiesTwo prospective interventional studies were assessed as being of low risk of bias [25, 30]. In total, 31 studies were assessed as being of moderate risk of bias, while 24 were high risk of bias.
Almost all studies clearly stated their aims; however, other items in the MINORS instrument were frequently absent, not reported or inadequate. Many studies inferred that consecutive patients were included; however, this was usually inadequately described. Almost half of the studies included at least some prospectively collected data. The specific focus of the included studies was very varied, and hence, the endpoints were quite heterogeneous. Most studies included important endpoint measures such as infections and severe adverse events; however, others had very minimal safety data. Blinded evaluation of study endpoints was very uncommon in the included studies. Over half of the included studies had a follow-up period of less than 2 years; while this was suitable for some study endpoints, it was deemed insufficient for some important outcomes. Few studies specifically commented on patients lost to follow-up, and no study prospectively calculated required study size to detect relevant safety outcomes.
3.4 Safety Results of Individual Studies and Results of Syntheses3.4.1 InfectionsInfections were the most commonly reported adverse event, and all but eight of the included studies specifically presented data on infections. Methods of reporting and categorising infection were very varied. Rates of infection, overall and for specific infectious syndromes, also varied considerably between studies. Similar to that seen with other bDMARDs in children, most infections were mild, and severe infections were often observed in patients with prior or concomitant immunosuppressive therapy. Notably, no substantive signal has emerged for opportunistic infections that was not identified in the original anakinra registration studies [31].
Upper respiratory tract infections, including nasopharyngitis, rhinitis, tonsillitis and sinusitis, were the most commonly reported type of infection. Other frequently reported infections included gastroenteritis, urinary tract infections, lower respiratory tract infections, cellulitis and lymphadenitis.
Viral infections were common overall but often undifferentiated. Influenza was the most commonly reported viral pathogen. Cases of other common childhood viral infections including varicella [9, 15, 16, 23, 32], Epstein–Barr virus [9, 13, 17, 33,34,35] and cytomegalovirus [15, 32, 36] were also reported.
Streptococcal infection (mainly pharyngitis) was reported by several studies [9, 16, 26, 27, 30]. Staphylococcal infection was reported infrequently but included one case of peritonitis [37] and sepsis [15]. One study reported two deaths from Gram-negative sepsis [38]. Few fungal skin infections and a single case of fungal peritonitis were reported [37].
Several studies looked at the risk of tuberculosis infection in endemic areas. Two Turkish studies reported high rates of latent tuberculosis infection prior to and during treatment with canakinumab for a range of autoinflammatory conditions; however, no episodes of active Mycobacterium tuberculosis infection were observed [39, 40]. Another Turkish study reported two lung tuberculosis infections in children on canakinumab for SJIA [41].
A minority of studies reported an absence of any observed infections, including a relatively large retrospective cohort study of children with SJIA (n = 61) on anakinra treatment [29].
3.4.2 MalignanciesMalignancy outcomes were specifically reported in 12 studies, of which, seven reported no cases of malignancy in their cohorts. A total of seven events were recorded, although two reports of a patient with acute myeloid leukaemia (AML) may overlap [20, 22]. Observed malignancies often occurred after anti-IL-1 therapy discontinuation and were often deemed to be unrelated to the anti-IL-1 medication. Notably, follow-up was variable and therefore may not consistently capture all long-term risk, although registry and long-term extension data demonstrate no applicable signals.
Haematological malignancies were the most common; three cases of AML were reported [13, 20, 22]. One patient receiving canakinumab for FMF was diagnosed with AML, and canakinumab treatment was discontinued [13]. Another patient was a female who had received anakinra at the age of 9 months for SJIA. She had developed severe macrophage activation syndrome (MAS) during her anakinra treatment, which was treated with steroids, cyclosporin A and etoposide. She developed AML at the age of 4 years and reached remission after allogeneic stem cell transplantation from a family donor [22]. A third patient was diagnosed with myeloid leukaemia 3 years after the last anakinra dose for SJIA. This patient had developed MAS during their anakinra therapy, leading to cessation of anti IL-1 therapy. As a result, the leukaemia was considered to be unrelated to the anakinra treatment [20]. The second and third patients were both from the BIKER registry with several overlapping clinical details suggesting the two reports may refer to the same individual [20, 22].
In total, two cases of lymphoma and one case of an ovarian mass were detected in a large Turkish study looking at the use of canakinumab for a range of paediatric rheumatic diseases [42].
One additional case of anaplastic large cell lymphoma was diagnosed after 113 days of canakinumab treatment for SJIA. The authors determined that the initial articular symptoms and fever were likely paraneoplastic manifestations resulting in an incorrect diagnosis of SJIA. This diagnosis was therefore considered unlikely to be related to canakinumab [15].
3.4.3 Interstitial Lung Disease (ILD)A total of eight studies reported on significant non-infectious respiratory pathology such as interstitial lung disease (ILD) in anti-IL-1-treated patients. All of these events were reported in patients with SJIA, except for one patient with an unclear diagnosis in a cohort consisting of multiple childhood rheumatic diseases (including SJIA) [42].
Overall, three were cases of interstitial lung disease [42,43,44]. Two of these cases were associated with canakinumab [42, 44], while the other patient had received anakinra [43]. One of these patients on canakinumab for an unknown indication developed ILD and drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome [42]. The other patient on canakinumab for SJIA was reported to have only mild ILD [44]. One patient reportedly had ILD after receiving treatment with anakinra for SJIA for over 24 months [43].
There were another four patients with potentially similar pathology. One patient had MAS and pulmonary fibrosis after treatment with rilonacept for SJIA; however, this was assessed as not related to the drug by treating physicians [45]. There was one case of prolonged eosinophilia with anakinra therapy for SJIA with “associated lung involvement” [46]. In a study on canakinumab for SJIA, there was one death related to lung injury in a patient with MAS events complicated by pulmonary hypertension and interstitial pneumonia [16]. Another patient in the same study had developed acute interstitial pneumonitis and transfusion-related lung injury, which resolved spontaneously but led to the patient discontinuing the study [16].
There were two cases of pulmonary alveolar proteinosis, a high-risk lung condition which more recently has been observed to occur in patients with SJIA with severe disease [47, 48]. One severe case developed in the context of canakinumab therapy in a patient with SJIA that led to study discontinuation for that individual [44]. A second patient was a 17-month-old female with treatment-refractory SJIA and smouldering MAS who had received treatment with both anti-IL6 and anti-IL1 blockade, in addition to cyclosporine, before progressing to etoposide as a bridge to allogeneic haematopoietic stem cell transplantation [49].
Another patient with SJIA in the same study had patchy ground glass changes bi-basally at diagnosis and achieved remission and remained off all treatment within 2.7 years after being commenced on anakinra within 3 months of diagnosis [49].
3.4.4 Drug Reactions
Comments (0)