
Remember me


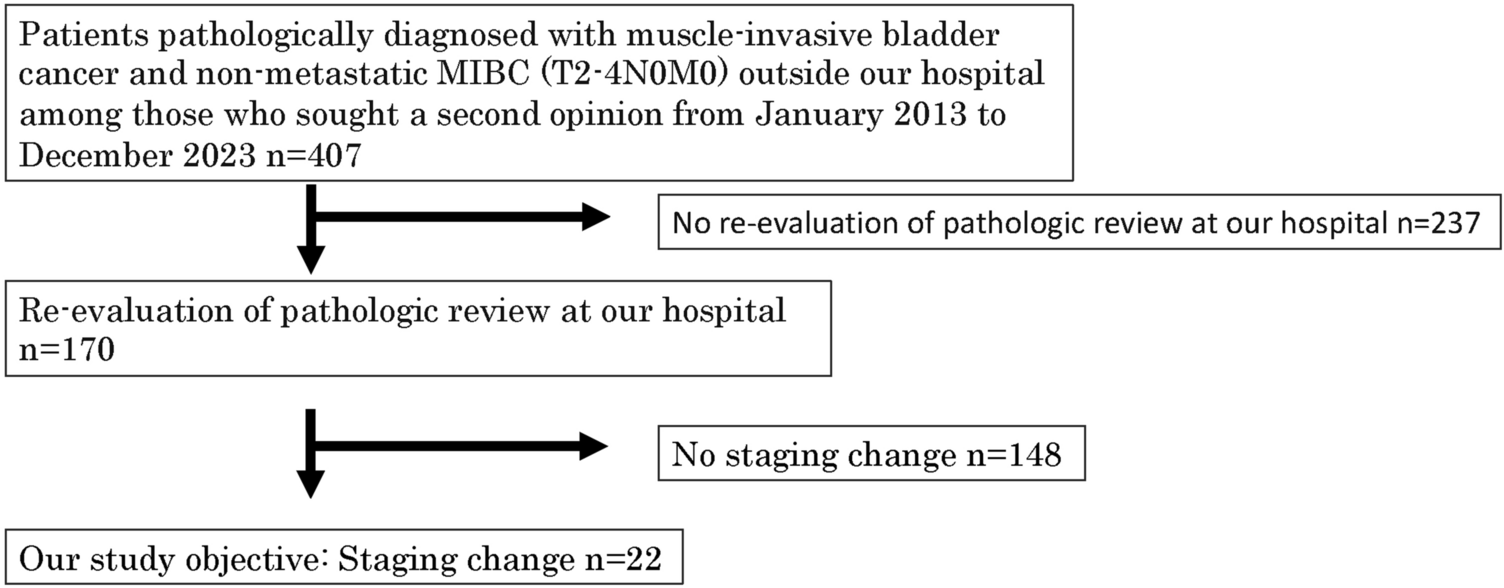
During the study period, 407 patients were diagnosed with MIBC based on pathology at other institutions and sought consultation at our hospital's outpatient department for a second opinion. Of the 407 patients who visited for a second opinion, 170 chose to continue care at our hospital. The remaining patients likely continued treatment at their original institutions due to geographic, social, or relational factors, although these reasons were not uniformly documented. These 170 patients desired evaluation and treatment at our hospital and underwent re-examination of their pathological diagnosis obtained from the referral hospital. Muscle invasion was not determined, and the pathological stage changed in 22 (12.9%) patients during pathological re-examination (Fig. 1).
Fig. 1
All cases were histologically diagnosed as urothelial carcinoma, and no variant histologies. Six patients were diagnosed with Ta. Among them, three had muscularis propria in their samples, two did not, and in one case, the sampling was uncertain. In addition, 16 patients were diagnosed with T1, of which nine had muscularis propria, two did not, and five had uncertain sampling. In the five patients who had uncertain sampling, the pathologists had difficulty distinguishing between the muscularis propria and muscularis mucosae, with uncertainty or significant crush artifacts, which made it unclear whether the muscularis propria was present (Table 1).
Table 1 Tumor characteristics of patients with stage changesMRI was performed before TUR in 11 of the 22 patients. In the 10 cases for which MR images were available, vesical imaging reporting and data system (VI-RADS) evaluation showed that one patient had a score of 1, three had a score of 2, and six had a score of 3. None of the patients had VI-RADS scores of 4 or 5. Twenty-two patients had solitary tumors measuring < 2 cm (Table 1).
Factors influencing discrepancies in the pathological stagingFactors influencing discrepancies in pathological staging were examined in terms of treatment time and referral hospital type. When divided into two treatment periods, 2013–2016 and 2017–2023, the rates of discrepancy in pathological stage were 14% (11/80) for 2013–2016 and 12.2% (11/90) for 2017–2023. Regarding the type of referral hospital, the discrepancy rate for the pathological stage in patients referred from university hospitals or cancer centers was 6.9% (4/58), whereas that in patients referred from community hospitals was 16.0% (18/112).
Treatment changes according to the re-evaluation of pathologyOf the 22 cases with discordant results, immediate radical cystectomy was proposed for 4 patients, with 3 patients undergoing treatment at our hospital and 1 receiving treatment at the referral hospital. Eighteen patients were re-evaluated using TUR at our hospital (Table 2).
Table 2 Results of TUR evaluation and treatment changeThe pathological results of TUR evaluation were as follows: among the five patients who were pathologically re-evaluated as having Ta, the results of TUR evaluation were as follows: three patients with T0, one patient each with Ta and Tis, and none with T2 or T13. Among the seven patients who were pathologically re-evaluated as having T1 or higher (without muscularis propria sampling or uncertain), the results of TUR evaluation were as follows: four patients with T0, two with T2, one with Tis, and none with T1 or Ta. Among the six patients who were pathologically re-evaluated as having T1 (with muscularis propria sampling), the results of TUR evaluation were as follows: three patients with T0, two with Tis, one with T2, and none with T1 or Ta (Table 2).
The pathological results of the TUR evaluation led to the following treatment recommendations: radical cystectomy was offered to one patient, radiation therapy to six, intravesical Bacillus Calmette-Guérin (BCG) instillation to nine, and observation to two. Eleven patients were treated for NMIBC, and 6.5% (11/170) required treatment modifications.
Prognosis of patients with pathologically discordant casesOf the 11 patients who underwent radical cystectomy or radiation therapy (4 patients without TUR evaluation and 7 with TUR evaluation), during a median follow-up period of 41 months (range, 2–113 months), 9 had no evidence of disease, and 2 had distant metastatic recurrence (Table 3).
Table 3 Prognosis of patients with treatment changesOf the nine patients who received BCG therapy and two patients who underwent observation during a median follow-up period of 36 months (range, 1–102 months), eight patients had no evidence of disease, two had Ta intravesical recurrence, and one had lung metastasis despite no intravesical recurrence.
Comments (0)