Recently published studies have analyzed MAUDE-reported AEs but have focused on specific procedures or diagnoses [13, 16, 17]. Ours is the first comparing MAUDE-reported AEs between TFLs and Ho: YAG lasers across all urologic procedures. We found most AEs did not involve patient events (86.5% in TFL, 64.7% in Ho: YAG), and TFLs were associated with fewer patient-involved events (p < 0.0001).
Most Ho: YAG laser device-related events were device or laser fiber malfunctions (44.4%), followed by fiber breaks (38.2%). A 2014 MAUDE-based study similarly found 46% of Ho: YAG-related AEs involving fiber breakage or device failure, although more recently Juliebø-Jones et al. reported an even higher rate (78.8%) of fiber breakage [12, 13]. However, neither study included TFLs, which we found had significantly higher fiber breakage rates both overall (57%) and in non-prostate procedures. Consequently, there were also significantly more breakages inside patients with TFLs. This may be related to their thinner diameter compared to Ho: YAG, though altogether these results show that laser fibers—especially TFLs—are fragile and careful handling could mitigate risk [5]. Additionally, differences in generator power output may contribute to the observed variation in fiber-related events.
Ho: YAG lasers had significantly more Level II events, most being cancelled or aborted procedures (147/194) which, compared to another study analyzing MAUDE Ho: YAG events, our rate was notably higher (30.2% vs. 5.2%) [13]. This discrepancy could be explained by their focus on lithotripsy procedures, while we included all laser-related procedures. Conversely, their study reported a higher incidence of prolonged anesthesia (14.7%) compared to ours (0.6%), possibly due to more complex cases in their sample or differing definitions. Prolonged anesthesia may reflect equipment troubleshooting, bringing in backup machines or even retrieving fiber pieces. Aborted or changed procedures might also indicate inappropriate treatment indications and could be underreported or not explicitly stated.
Level III events were significantly more common in TFLs, although the number was small (10 AEs; 2.1%). These included two ureteral perforations (one from a fiber break), one renal perforation, one case of intrarenal bleeding, four patients requiring additional procedures (two resulting from fiber breakage), one procedure reportedly prolonged for 7 h due to malfunction of the machine, and one patient whose approach was changed due to an unknown machine error. Ho: YAG laser Level III AEs included one additional procedure and an intrarenal injury (both secondary to fiber breaks), and a ureteral perforation without an identified device event.
Our findings align with Chandramohan et al.’s study reporting a significantly higher rate of mucosal injury with TFL use (28.8%) compared to Ho: YAG lasers (11.1%) during URS [19]. In contrast, a systematic review reported significantly lower rates of intraoperative complications with TFLs (OR 0.34), and a meta-analysis also found a lower incidence when compared to Ho: YAG lasers, though without statistical significance [20, 21]. Similarly, a randomized controlled trial reported fewer intraoperative complications with TFLs during URS [22]. However, most published data focus on a single procedure, whereas the MAUDE database—and consequently our study—covers a broader range of procedures.
Still, most events were Level I (83.9% TFL; 52.3% Ho: YAG), comparable to studies assessing device safety in urology. These have reported Level I rates ranging from 39.4% to as high as 99.3%, depending on devices and procedures included [15,16,17]. Others using the Clavien–Dindo classification to report outcomes have similarly found 82.5% of complications pertaining to grades I or II (mild) [14].
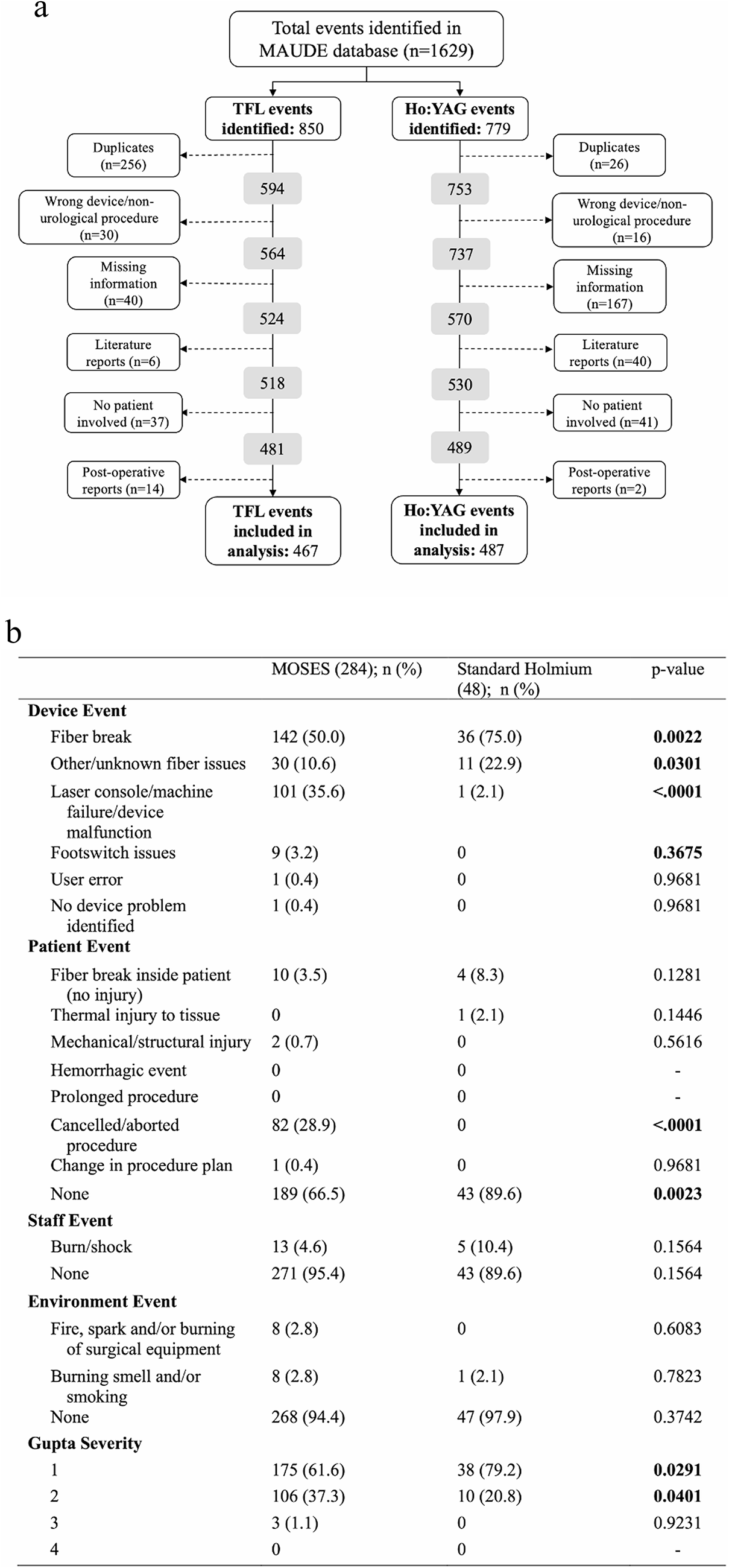
Stratification by procedure demonstrated no significant differences between lasers in prostate cases, which was somewhat expected given the small sample. In contrast, non-prostate procedures accounted for most reports, with events generally classified as Level I (73.6% TFL, 64.9% Ho: YAG). Within Ho: YAG lasers, stratification by pulse modulation suggested that MOSES may reduce fiber-related issues but was more often associated with console malfunctions and cancelled procedures compared to standard Ho: YAG. Most events in both groups were minor, though MOSES had relatively more Level II AEs. However, interpretation is limited by the relatively small number of standard Ho: YAG reports.
Additionally, after the August 2021 FDA TFL-device recall, a significantly greater proportion of events had no patient involvement (60.8% pre-recall vs. 90.3% post-recall), with a significant decrease in Level II and III events [11]. While Level III events were still reported post-recall (3 pre vs. 6 post), the overall reduction and increase in reports without patient harm suggest that the corrective actions had a positive impact, highlighting the importance of ongoing surveillance and adherence to laser safety protocols.
A critical principle in laser use is not surpassing the 43° C thermal threshold, as this can lead to tissue damage [23]. In vitro studies measuring intraureteral fluid have shown high temperatures with laser use, one even reporting higher maximum temperatures with TFLs than Ho: YAG lasers [24]. Gupta et al. recently measured intrarenal temperatures during endoscopic procedures (20 patients), revealing both Ho: YAG and TFLs quickly reached high temperatures at high-power settings, though TFLs reached significantly higher maximum temperatures during “pop-dusting.” [25] In addition to intrarenal fluid temperature, factors such as thermal safety distance (thermal dose + laser fiber tip distance) and exposure duration also contribute to thermal injury risk [26]. Strategies including ureteral access sheaths, continuous irrigation, and intermittent laser activation can help mitigate these effects [26, 27].
We found no statistically significant differences in thermal or structural tissue injuries; however, there were three reports of thermal injury with TFLs, while the two reported with Ho: YAG lasers were skin burns. We also found two ureteral and one intrarenal perforation in the TFL group, compared to one ureteral, one intrarenal, and one bladder perforation in the Ho: YAG group. The bladder perforation— the only Level IV AE— occurred during a holmium laser enucleation of the prostate. Reportedly there was gas explosion with bladder rupture requiring conversion to open surgery; one hour later, the patient’s blood pressure dropped, acute myocardial infarction was diagnosed, and the patient ultimately died.
In addition to intraoperative complications, long-term issues such as ureteral strictures have been reported, with Para et al. noting a significantly higher incidence following TFL use compared to Ho: YAG during URS (11/238 vs. 4/240, respectively) [28]. In a separate study, Villani et al. compared manufacturer-recommended versus individualized TFL presets and reported a significantly higher stricture rate with the former (11% vs. 1%) [29]. Although we didn’t specifically analyze this complication, several reports in our MAUDE dataset mentioned stricture-related events. However, because of limited procedure details, lack of follow-up, and delayed nature of stricture development, these events could not be reliably assessed or linked to intraoperative laser use. Still, their presence suggests the potential for thermal injury even when using strategies like power settings adjustment or continuous irrigation [23, 24, 28]. Further research is needed to better characterize these complications.
Our study has limitations. The MAUDE database depends on voluntary reporting and is subject to reporting bias. The total number of cases is unknown, preventing incidence calculation, and specific details such as procedure type, laser settings (frequency, power, pulse modulation) and use of adjunctive measures are often missing. Follow-up information is rarely provided, making it difficult to establish causality, and postoperative outcomes such as fever, stone-free rates, and strictures are not reliably captured, limiting assessment of delayed complications. Despite this, we believe our study offers an insight into laser AEs and their overall safety in urology.



Comments (0)