
Remember me


Women ≥ 18 years old with apical or anterior POP (POP-Q stage III/IV) who required surgical correction were included. The exclusion criteria comprised POP-Q stages I and II, asymptomatic prolapse, pregnancy, planned childbearing, significant comorbidities (e.g., uncontrolled diabetes, infections, pelvic radiation, pelvic cancer) or POP without functional impairment, diminished leg mobility issues, cognitive impairment, mesh/glue allergies, lack of insurance, or legal guardianship. The eligibility was assessed by the gynecological surgeon. All participants provided written informed consent.
Randomization and blindingPatients were randomized to a 1:1 ratio using a computerized system. All surgeries were performed by the same experienced surgeon who had performed more than 30 prior procedures using a standardized laparoscopic approach [7]. In the glue group, laparoscopic sacrocolpopexy was performed using the synthetic glue Ifabond™ and in the sutures group, the procedure was performed using surgical suturing for mesh fixation. Randomization was blinded.
Surgical procedureAll patients underwent laparoscopic sacrocolpopexy using a standardized technique using polypropylene mesh (Parietex ™, Covidien, Mansfield, MA) [8]. Anterior and posterior meshes were fixed with either Ifabond™ glue or non-absorbable sutures. Separate anterior and posterior meshes were used when appropriate, no Y-shaped mesh was applied. Patients with stage II rectocele and/or symptoms of dyschezia were candidates for posterior mesh fixation.
For the patients with mesh fixation using glue, a 1.5mL vial was needed for each procedure. The posterior mesh was fixated by applying four drops of 0.2mL of glue on the lower, middle, and upper posterior vaginal wall as laterally as possible [2, 8] and then to the levator ani muscles. The anterior mesh was fixated on the anterior surface of the vagina by instilling glue in a dropwise fashion on six to nine points, with a 0.5 cm minimum distance between two points [8] (see Video in supplementary material).
In all cases, Ifabond™ vaginal mesh adhesive (Peters, France) was used, with the same application technique. In contrast, in the patients randomized to the mesh fixation through suturing, fixation of the posterior mesh was performed via applying three non-absorbable polyethylene terephthalatesutures (Mersuture™) on the same points, and by applying an average of seven nonabsorbable sutures on the anterior vaginal wall.
The mesh was fixed to the sacrum using sutures in both groups. Peritoneum was closed to retroperitonealize the mesh. No tacker or clip were used. The same experienced surgeon with more than 30 procedures who has already reached the learning curve performed all laparoscopic sacrocolpopexies in both groups.
Physical and chemical properties of the cyanoacrylate glueIfabond™ is a synthetic sterile, translucent, non-toxic cyanoacrylate tissue adhesive (manufactured by Fimed S.A.S.; CE label, class III) approved for internal use. This low-viscosity glue is sterilized by beta radiation. Upon application to living tissue, it rapidly polymerizes into the flexible adhesive poly n-hexyl-cyanoacrylate [9]. The polymer degrades enzymatically through hydrolysis, producing formaldehyde, hexanol, and cyanoacetic acid. The rate of degradation is inversely proportional to the polymer chain length.
In an animal model, wall reinforcement integrated with tissue more quickly when secured with glue compared to sutures [10]. Tissue formation through cellular colonization occurs around the glue fixation points, allowing the reinforcement to integrate [10]. In a rabbit model, Bellon et al. observed a significantly greater macrophage count between 14 and 90 days following PTFE (polytetrafluoroethylene) reinforcement secured with Ifabond™. Similarly, in a sheep model, the inflammatory response—characterized by increased lymphocyte and plasma cell activity—was significantly greater at two weeks using Ifabond™ compared to staples [11]. Additionally, the apoptotic cell count at 90 days was significantly higher with Ifabond™ than with octyl cyanoacrylate. These responses contributed to significantly stronger fixation at both 14 and 90 days using Ifabond™ [10]. The inflammatory reaction induced by the fixation method, along with the wall reinforcement, supports effective mesh anchorage without causing vaginal ulceration [12].
Data collectionPre-, intra-, and post-operative data were collected by the operating surgeon. Patients completed validated questionnaires (PFDI-20, PFIQ-7, PISQ-12, VAS) preoperatively and at 1, 12, and 24 months post-operatively. Anatomical success was defined as POP-Q ≤ 1, and functional success was defined as the absence of bulge symptoms (PFDI-20, Q3). Composite success required anatomical success, no additional surgery, and no bulge symptoms. Mesh shrinkage was defined through IUGA criteria [13]. Demographic and clinical baseline data were collected at enrolment (Table 1). Operative variables included operative time, blood loss, dissection/fixation duration, and complications (Table 2).
Table 1 Baseline characteristics of patientsTable 2 Perioperative outcomesStatistical analysisStatistical analysis was performed using SAS software (SAS Studio 3.8; SAS Institute Inc., Cary, NC, USA). Data did not follow a normal distribution (based on the results of the Shapiro-Wilk test), therefore quantitative results were expressed as median [range] and qualitative results as count and percentage. The variables were compared between both groups using the Mann-Whitney U test for quantitative data and Fisher’s test for qualitative data. The comparison between pre-op and post-op data was performed using the non-parametric Wilcoxon signed-rank test for paired series for quantitative data, and McNemar’s test for qualitative data. Statistical significance was defined as a p-value lower than 0.05.
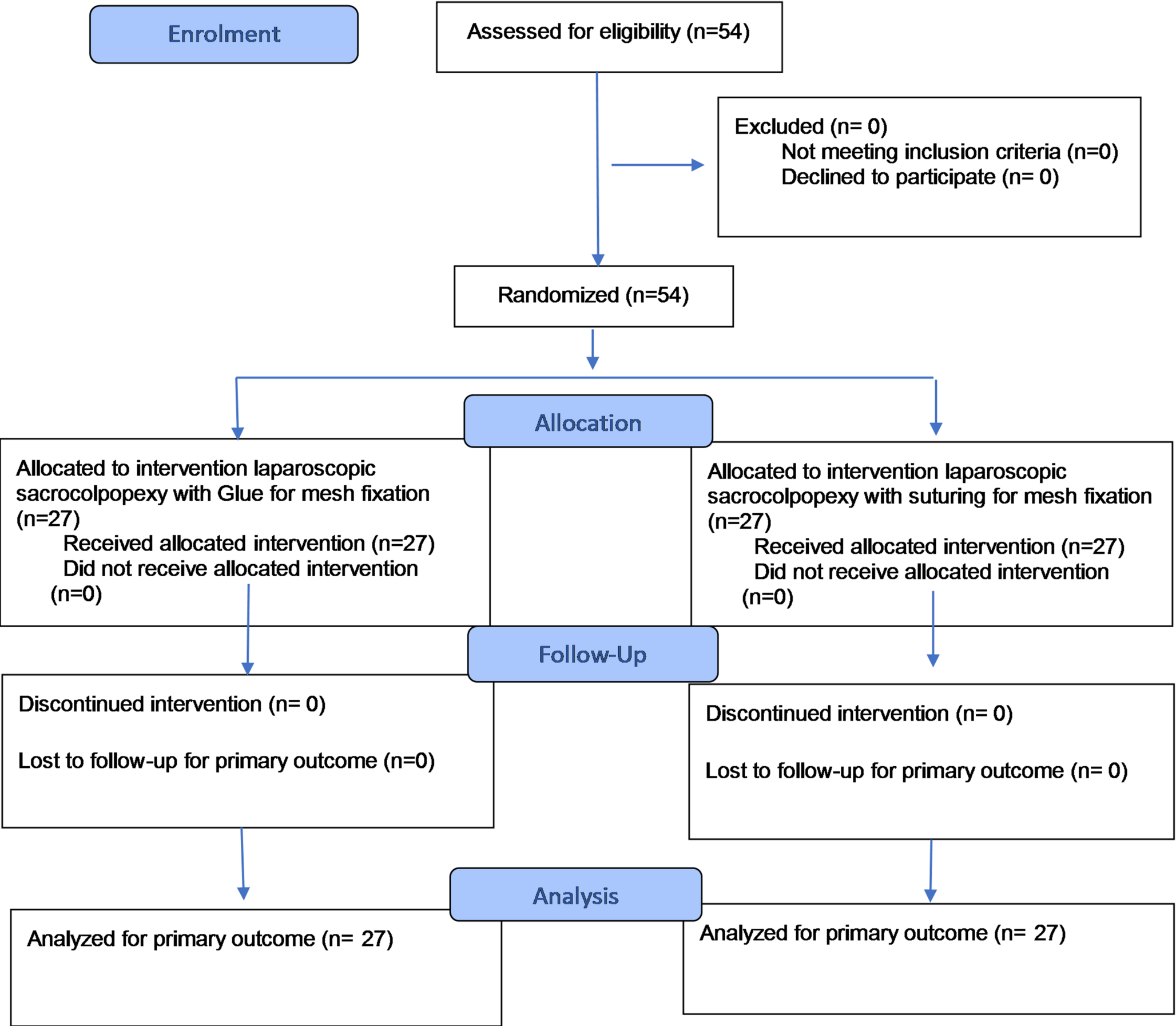
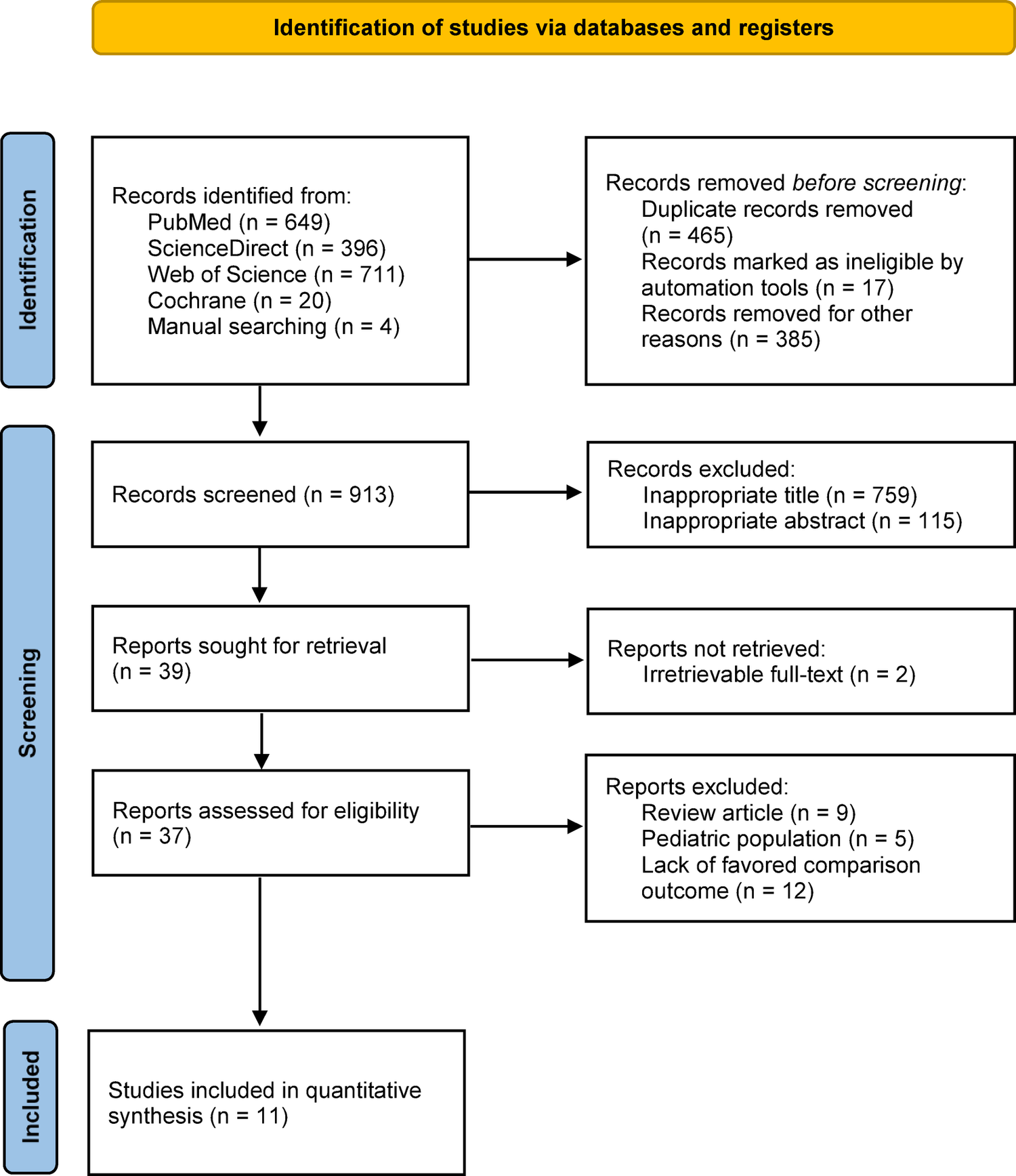
Sample size calculationIt was hypothesized that in the Ifabond™ group, the mean operative time was185 minutes [14]. In our previous study using Ifabond™, the mean operative time was 169 min with reduced operative time with every procedure over the course of the learning curve. Considering the slope of the trend line (a=-0.0248), it can be extrapolated that the operative time was decreased by approximately 10 min over the course of 12 months [2]. Therefore, it was hypothesized that the average operative time in the group treated with Ifabond™ adhesive would be approximately 160 min. Based on this assumption, to achieve an 80% statistical power with an alpha error of 5% and a standard deviation of 30 min, the required sample size is 24 subjects per group, i.e., 48 participants in total. Anticipating approximately 10% dropout prior to the assessment of the primary endpoint, we therefore included a total of 54 patients (as shown in Fig. 1).
Fig. 1
CONSORT 2025 Flow Diagram
Comments (0)