
Remember me


EUS has emerged as a valuable diagnostic tool in the evaluation and management of AIP, owing to its high sensitivity, ability to assess both —pancreas and surrounding structures— and its role in guiding tissue sampling for histological analysis. There are no pathognomonic EUS imaging findings of AIP.
Pancreatic findingsDiffuse AIPDiffuse pancreatic enlargement and altered echotexure is seen. Gland border is thickened and echogenic interlobular septa may be seen. There often is loss of normal salt and pepper pattern of the pancreas with bulky mildly hypoechoic parenchyma with hyperechoic strands seen within (Fig. 4). The MPD may appear narrowed, irregular with hyperechoic walls [19, 20]. Peri-pancreatic fluid collections are less common and not specific for AIP [20]. However, in rare cases, pseudocysts may be seen.
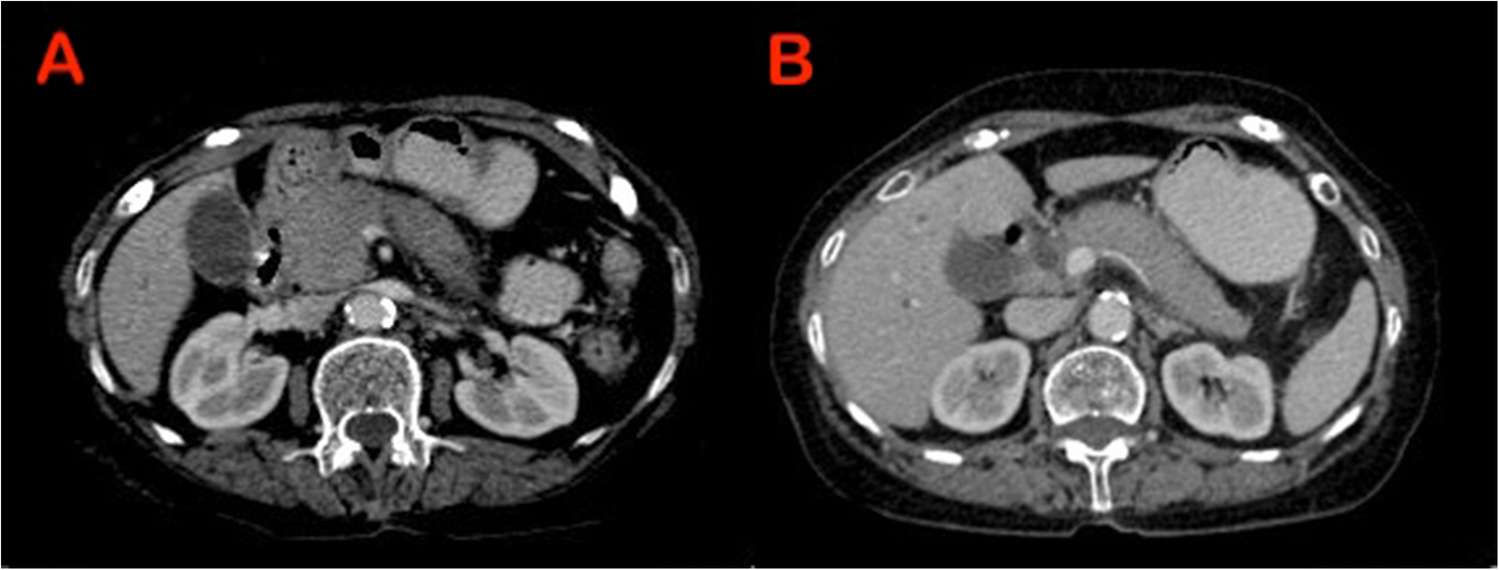
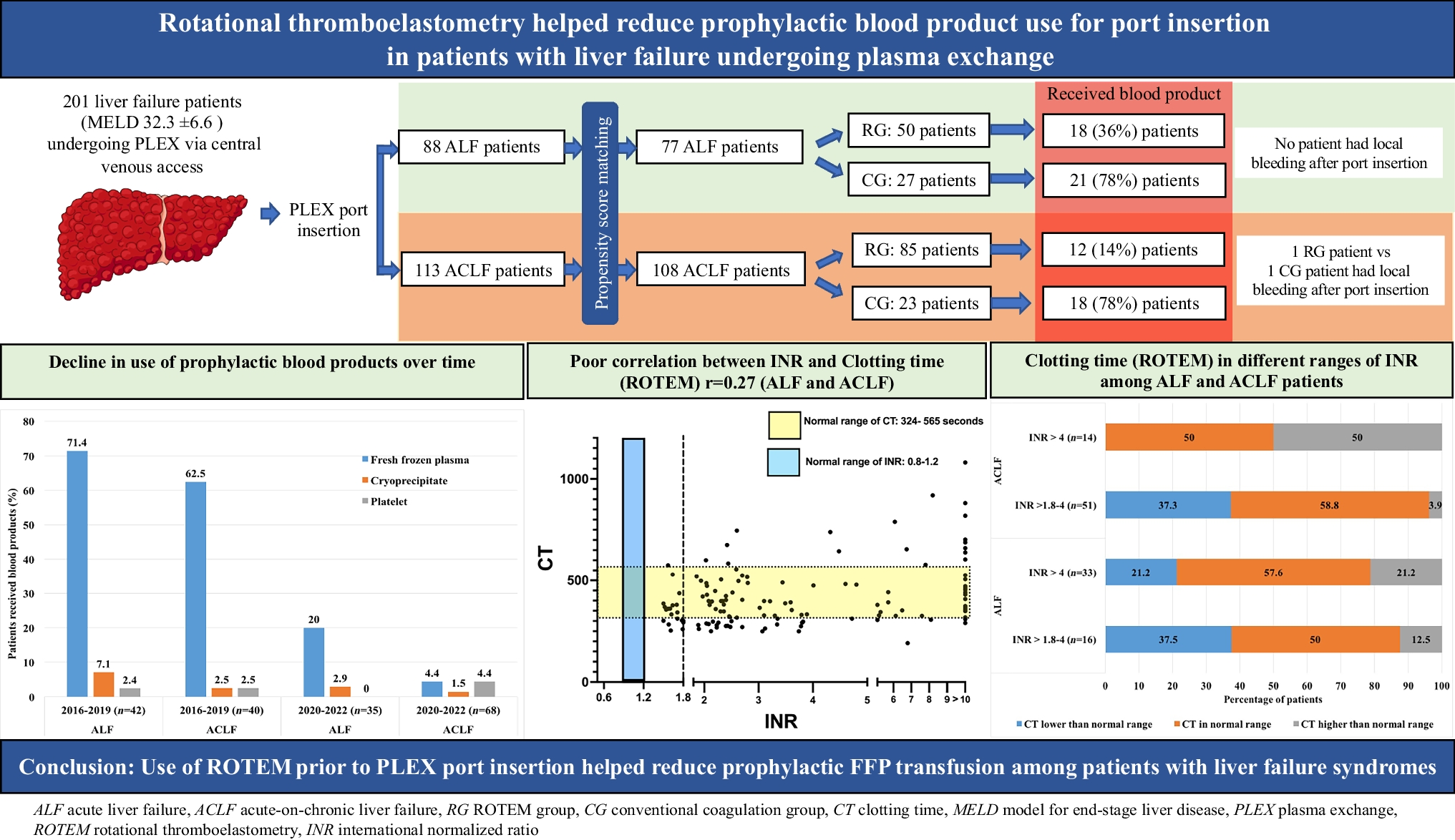
Fig. 4
(A) Pancreatic head showing heterogenous echogenicity with undilated pancreatic duct. (B) Diffuse thickening of the bile duct seen on endoscopic ultrasound. (C) Biopsy taken from the pancreatic body which also appears heterogeneously hypoechoic. (D) Enlarged sub-carinal lymph node which was reactive seen in association with autoimmune pancreatitis
Focal AIPFocal AIP can present as a solitary mass, often seen as a hypoechoic lesion, primarily located in the head of the pancreas. This mass may give the impression of invading nearby vessels and be associated with enlarged peri-pancreatic lymph nodes resembling locally advanced pancreatic cancer (PC) [19, 20]. The main pancreatic duct (MPD) wall may appear thickened, narrowed within the lesion. However, pancreatic duct cut-off sign is not seen [19, 20]. Despite well-established EUS features of AIP reported globally, there is a notable lack of data from Indian centres. In a previous study by Jain et al. [9], 41% patients were diagnosed using endoscopic ultrasound-guided biopsy. This gap highlights the critical need for robust, region-specific studies to validate these findings in the Indian context.
Other organ involvementThe biliary tree is the most common extra-pancreatic organ involvement in AIP and was found to affect 58% of patients in a Japanese survey [21]. EUS provides a comprehensive view of the entire common bile duct, helping to identify the cause for biliary strictures. A typical EUS feature of the common bile duct is homogeneous, regular thickening of the bile duct wall, known as the “sandwich-pattern”. This pattern is characterized by an echopoor intermediate layer with hyperechoic inner and outer layers (Fig. 3). Along with the bile duct, gallbladder wall thickening can also be seen in AIP [20, 22]. Intra-ductal ultrasonography (IDUS) can also be used during endoscopic retrograde cholangiography to assess biliary stenosis. Naitoh et al. studied IDUS in 23 IgG4-related sclerosing cholangitis (IgG4-SC) patients and found that circular, symmetric wall thickness with smooth margins and a homogeneous intermediate layer were more common in AIP than cholangiocarcinoma. Additionally, wall thickness in non-strictured areas of IgG4-SC was greater than in Cholangiocarcinoma, with a thickness over 0.8 mm suggesting IgG4-SC [23].
The reported frequency of lymphadenopathy in AIP patients varies widely across EUS studies, ranging from 31.2% to 72% [15, 24, 25]. Hilar lymphadenopathy is among the most commonly reported extra-pancreatic findings. Enlarged lymph nodes are also observed in the peri-pancreatic and celiac regions [21]. However, the conventional EUS criteria for predicting malignant lymph nodes such as size (> 1 cm in diameter on the short axis), hypoechoic appearance, round shape and smooth border may not be reliable in pancreato-biliary disorders, making it challenging to distinguish them from those associated with AIP based on EUS features alone [26, 27]. AIP can have vascular invasion of medium and large-sized vessels due to the inflammatory process. Peri-pancreatic vascular involvement is a common finding in AIP, detected in 44% to 67% of cases on CT. The most frequently observed vascular abnormalities include stenosis or occlusion of the splenic vein and/or superior mesenteric-portal vein, along with peri-gastric collateral formation [28,29,30]. In a study of 14 AIP patients, EUS suspected portal or mesenteric vein invasion in 21% of cases, compared to 14% on CT. Notably, none of these patients developed pancreatic cancer during follow-up [19].
Staging of the diseaseAIP is classified into early-stage disease, which is characterized by a good response to corticosteroid therapy and advanced-stage disease, which is marked by stone and cyst formation resembling findings in chronic alcoholic pancreatitis [31, 32]. EUS can help differentiate between the stages of AIP. Kubota et al. [33] demonstrated that lobularity and a hyperechoic pancreatic duct margin are characteristic EUS features of early AIP, compared to advanced AIP.
To differentiate from pancreatic cancerAIP constitutes a significant portion of pancreatic resections performed for suspected malignancy. In two surgical series, AIP accounted for 19.5% and 23.4%, respectively, of all cases where benign disease was diagnosed following pancreatic resection performed for suspected malignancy [34, 35]. In an Indian study, AIP was initially misdiagnosed as pancreatic cancer due to overlapping clinical and imaging features [6]. In another series of IgG4-related gastrointestinal disease, one-third of cases were diagnosed after surgery, most of which were autoimmune pancreatitis [36]. Therefore, correctly diagnosing focal AIP and distinguishing it from PC is crucial, although it is challenging due to overlapping clinical and imaging features. In a study by Guo et al., EUS features for focal AIP included diffuse hypoechogenicity, hyperechoic foci, bile duct wall thickening and peripancreatic hypoechoic margins. In contrast, PC showed focal hypoechogenicity, absence of parenchymal heterogeneity, pancreatic duct dilation and vessel involvement. The model demonstrated excellent diagnostic accuracy, with sensitivity ranging from 83.7% to 91.8% and specificity from 93.3% to 95.6% [25]. Tacelli et al. [37] suggested that thickened pancreatic and bile duct walls, an elastic pattern and the absence of vessel infiltration were found to independently support the diagnosis of focal AIP1 over PC. Along with conventional EUS features, advanced EUS modalities such as EUS elastography and contrast-enhanced EUS (CE-EUS) can aid in diagnosing AIP and differentiating between focal AIP and PC. Table 2 summarizes the findings comparing AIP and pancreatic cancer.
Table 2 Differentiating autoimmune pancreatitis from pancreatic cancer using endoscopic ultrasound modalitiesEUS elastographyEUS elastography assesses the elasticity of pancreatic tissue, with regions of increased stiffness potentially indicating fibrosis, a characteristic feature of AIP. There are two main types of EUS elastography: strain elastography and shear-wave elastography (SWE). Strain elastography assesses tissue stiffness by measuring relative deformation in response to external or internal pressure, displaying results as a color-coded map. In AIP, qualitative elastography shows an inflamed area with a predominantly green pattern and slight red or yellow lines, while normal parenchyma appears uniformly green (Fig. 5) [38]. Elastography may also help differentiate AIP from PC, as AIP shows a diffuse stiffness increase, while PC has localized stiffness [39]. However, it is semi-quantitative and depends on subjective image selection.
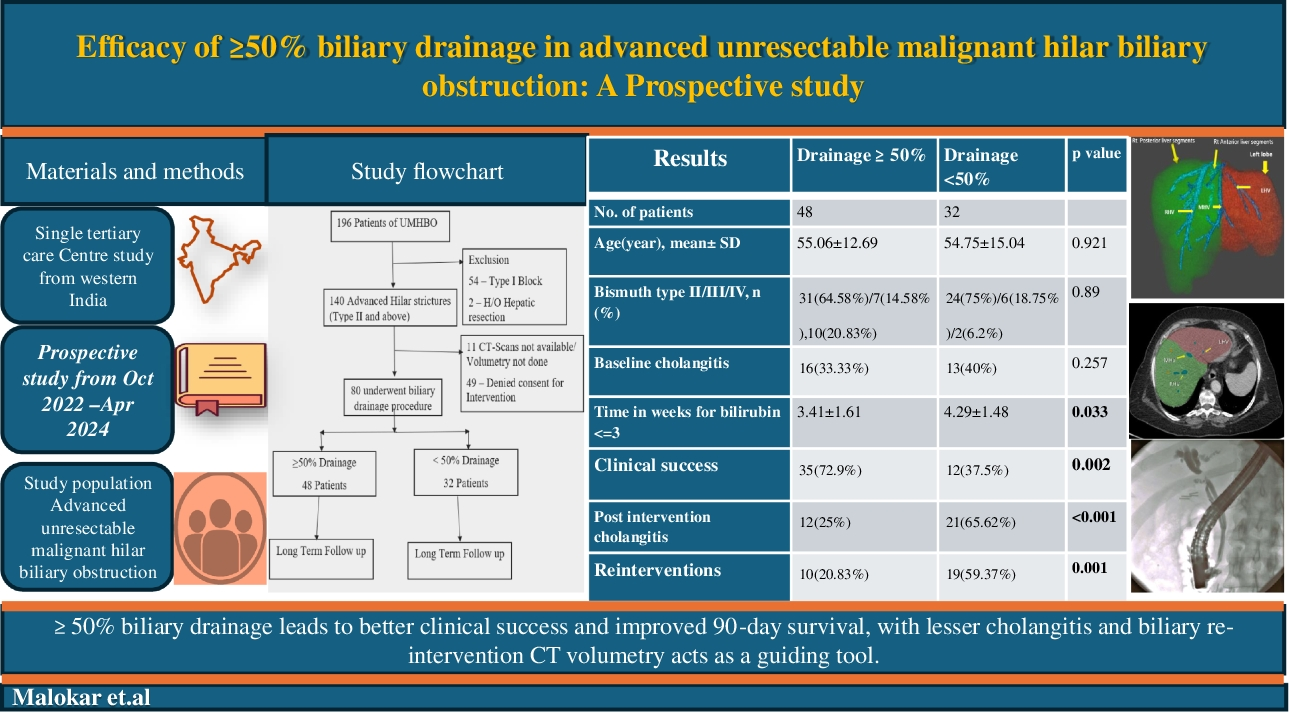
Fig. 5
Endoscopic ultrasound showing heterogenous parenchymal echogenicity of the pancreas (left panel); On strain elastography the parenchyma appears diffusely firm (right panel)
In contrast, SWE generates shear waves within the tissue and measures their propagation speed to provide absolute elasticity values, offering a more objective and reproducible assessment. A study evaluated the feasibility and clinical utility of EUS shear-wave elastography (EUS-SWE) in diagnosing and monitoring AIP. Tissue elasticity was measured in 160 patients, including 14 with AIP. EUS-SWE had a 97.6% success rate, with the median shear-wave velocity (Vs) in AIP patients (2.57 m/s) significantly higher than in normal controls (1.89 m/s, p = 0.0185). Steroid therapy reduced Vs from 3.32 to 2.46 m/s (p = 0.0234). The study concluded that EUS-SWM is a feasible and reliable tool for diagnosing AIP and assessing treatment response [40].
Contrast-enhanced EUS (CE-EUS)CE-EUS is an advanced imaging technique that enhances the evaluation of pancreatic lesions by providing real-time visualization of microvasculature and tissue perfusion. Its sub-type, contrast-enhanced harmonic EUS (CH-EUS) offers clear, real-time imaging of blood vessels in the target tissue, without artifacts commonly seen with Doppler mode. Additionally, CH-EUS enables the creation of time-intensity curves (TICs) and graphing of the changes in brightness over time through contrast [41]. A study by Cho et al. assessed the usefulness of CH-EUS in differentiating focal AIP from PC. Among 80 patients, focal AIP showed significantly higher rates of hyper to iso-enhancement (89% vs. 13%), homogeneous contrast distribution (81% vs. 17%) and absence of irregular vessels (85% vs. 30%) compared to PC (all p < 0.05). Combining CH-EUS features improved specificity to 94%. These findings suggest CH-EUS is a valuable non-invasive tool for distinguishing f-AIP from PC [42].
In another study by Dong et al. [43], CE-EUS helped differentiate AIP from PC. Among 60 AIP and 16 PC cases, AIP lesions showed iso or hyperenhancement, while PC lesions were mostly hypoenhancing (p < 0.01). Similarly, Ishikawa et al. investigated the role of CE-EUS in differentiating AIP from PC. Among 36 AIP and 36 PC patients, key EUS findings included hyperechoic areas in AIP and anechoic areas in PC, with PC exhibiting clearer borders and greater MPD dilation. CE-EUS revealed persistent enhancement in AIP (75%) and rapid contrast washout in PC (75%), achieving 75% sensitivity and 100% specificity. These results highlight the diagnostic value of EUS combined with CE-EUS in distinguishing AIP from PC [44].
A study by Imazu et al. evaluated whether quantitative perfusion analysis using the “Time Intensity Curve” (TIC) with CH-EUS can differentiate AIP from PC. TIC analysis in eight AIP and 22 PC patients showed significantly higher peak intensity (PI) and maximum intensity gain (MIG) in AIP. An MIG cut-off of 12.5 demonstrated high sensitivity and specificity. Thus, CH-EUS with TIC may improve the accuracy of distinguishing AIP from PC [45]. However, TIC analysis can be challenging as it requires precise techniques, specialized software and careful selection of the region of interest (ROI) to ensure accurate results. Another study by Ishikawa et al. evaluated a simplified multiphase CE-EUS method for differentiating pancreatic solid lesions without relying on a time-intensity curve (TIC). Among 210 patients, including 142 with PC, lesion enhancement patterns at 20, 40 and 60 seconds post-contrast were analyzed. Most PC cases showed an early enhancement followed by a hypovascular pattern, achieving 83.1% sensitivity, 86.8% specificity and 84.3% accuracy. Histopathological differences in tumor infiltration and neural invasion were noted. These findings suggest that multiphase CE-EUS is a practical and effective alternative to TIC for diagnosing pancreatic lesions [28].
EUS-guided tissue samplingThe ICDC outline a multifaceted approach to diagnosing AIP. When imaging findings are characteristic, the diagnosis can often be made without histologic confirmation, allowing for prompt steroid therapy. However, in cases with atypical imaging or a mass-forming lesion, distinguishing AIP from PC becomes essential for determining the appropriate treatment. In such instances, pancreatic biopsy sampling serves as the gold standard for confirming AIP, distinguishing it from cancer and identifying whether it is Type-1 or Type-2 AIP [46].
EUS-guided fine needle aspiration (FNA) and fine needle biopsy (FNB) are commonly used for obtaining pancreatic tissue in suspected AIP, but their diagnostic performance differs. FNA, traditionally used for cytologic evaluation, often yields insufficient tissue for histopathologic assessment, limiting its utility in diagnosing AIP, which relies on architectural features such as storiform fibrosis and obliterative phlebitis. It can only evaluate one of the four diagnostic criteria (IgG4 + cells), which is insufficient for diagnosing AIP [47]. In contrast, FNB provides better-preserved core tissue samples, enhancing the ability to meet histologic criteria for AIP. Meta-analyses and comparative studies suggest that FNB has a significantly higher diagnostic yield than FNA while maintaining comparable safety profiles. Therefore, FNB is increasingly preferred over FNA for obtaining adequate histologic samples in AIP diagnosis (Fig. 5).
Yoon et al. conducted a meta-analysis to compare the efficacy of EUS-guided FNA and FNB in diagnosing AIP. Analyzing data from nine FNA studies (309 patients) and seven FNB studies (131 patients), they found that FNB had a significantly higher pooled diagnostic yield for level 1 or 2 histologic criteria of AIP (87.2% vs. 55.8%, p = 0.030), while histologic tissue procurement rates were similar between the two techniques (91.3% for FNA vs. 87.0% for FNB, p = 0.501). Adverse events were comparable between groups. Additionally, 19G needles had a superior diagnostic yield compared to 22G needles (88.9% vs. 60.6%, p = 0.023). These findings suggest that FNB may offer better diagnostic accuracy for AIP, highlighting the need for a standardized definition of histologic sample adequacy [48].
A recent meta-analysis by Facciorusso et al. evaluated the diagnostic performance of EUS-guided FNA and FNB in AIP across 15 studies with 631 patients. The overall diagnostic accuracy of EUS tissue acquisition was 54.7%, with FNB significantly outperforming FNA (63% vs. 45.7%, p < 0.001). FNB also provided a higher rate of level 1 histological diagnosis (44.2% vs. 21.9%, p < 0.001) and definitive histopathology (24.3% vs. 14.7%, p < 0.001). The procedure was safe, with less than 1% experiencing post-procedural acute pancreatitis. These findings highlight the modest overall accuracy of EUS-guided sampling in AIP, but support the superior diagnostic yield of FNB over FNA [49]. As a result, EUS-guided tissue acquisition is shifting from FNA to FNB. Initial reports on EUS-FNB utilized Tru-Cut biopsy needles; however, these are no longer available due to limited manoeuvrability. The first second-generation FNB device introduced was a side-fenestrated reverse-beveled needle, but it failed to show significant advantages over standard FNA. More recently, advanced FNB needles with forward-acquiring designs have been developed, including Franseen-tip, fork-tip, Menghini-type and side-fenestrated forward-cutting beveled needles. Studies have demonstrated that these new-generation FNB needles provide superior histologic and diagnostic yields compared to both traditional FNA and earlier reverse-beveled FNB needles for evaluating solid pancreatic lesions. A recent retrospective study by Takada et al. compared the diagnostic performance of three EUS-FNB needles (Franseen needle, Menghini-tip needle and Reverse-bevel needle) for solid pancreatic masses, finding the Franseen needle superior in histologic core procurement, sensitivity and accuracy [50]. Kurita et al. in their prospective, multicentre trial compared two EUS-FNB needles for diagnosing Type-1 AIP. Total 101 patients were evaluated using either a 22-gauge Franseen needle or a 20-gauge forward-bevel needle. The Franseen needle obtained significantly more high-power fields and diagnosed a higher percentage of patients with level 1 or 2 lymphoplasmacytic sclerosing pancreatitis (LPSP) (78% vs. 45%, p = 0.001). Given its superior performance, the 22-gauge Franseen needle is recommended for routine histologic diagnosis of Type-1 AIP [51]. While wet suction is said to be better than other suction techniques for tissue sampling of solid pancreatic lesions, there is no data available exclusively for a cohort of AIP [35]. Also since histopathology is a critical issue in diagnosis of AIP, macroscopic on-site examination (MOSE) appears more relevant than rapid on-site examination which usually only gives cytology [52]. Figure 6 summarizes the diagnostic algorithm for differentiating AIP and pancreatic cancer [53]. Ampullary biopsy can aid in diagnosing AIP, especially when serum IgG4 is normal or pancreatic tissue is inaccessible. IgG4-positive staining (> 10 cells/HPF) shows good specificity (89% to 100%) for AIP and the procedure is safe with no major reported complications. The ICDC recommends ampullary biopsy during endoscopic retrograde cholangiopancreatography (ERCP) when AIP is suspected [54].
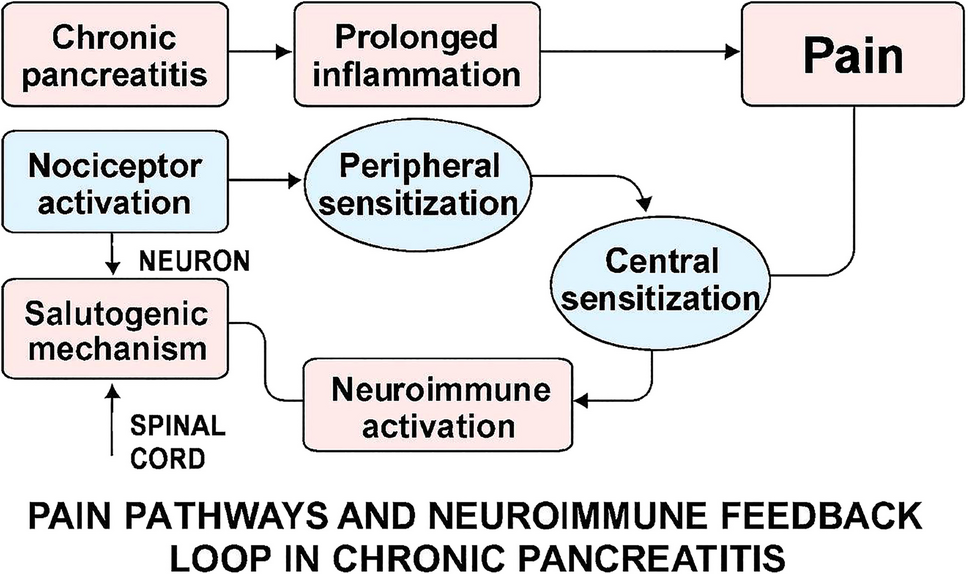
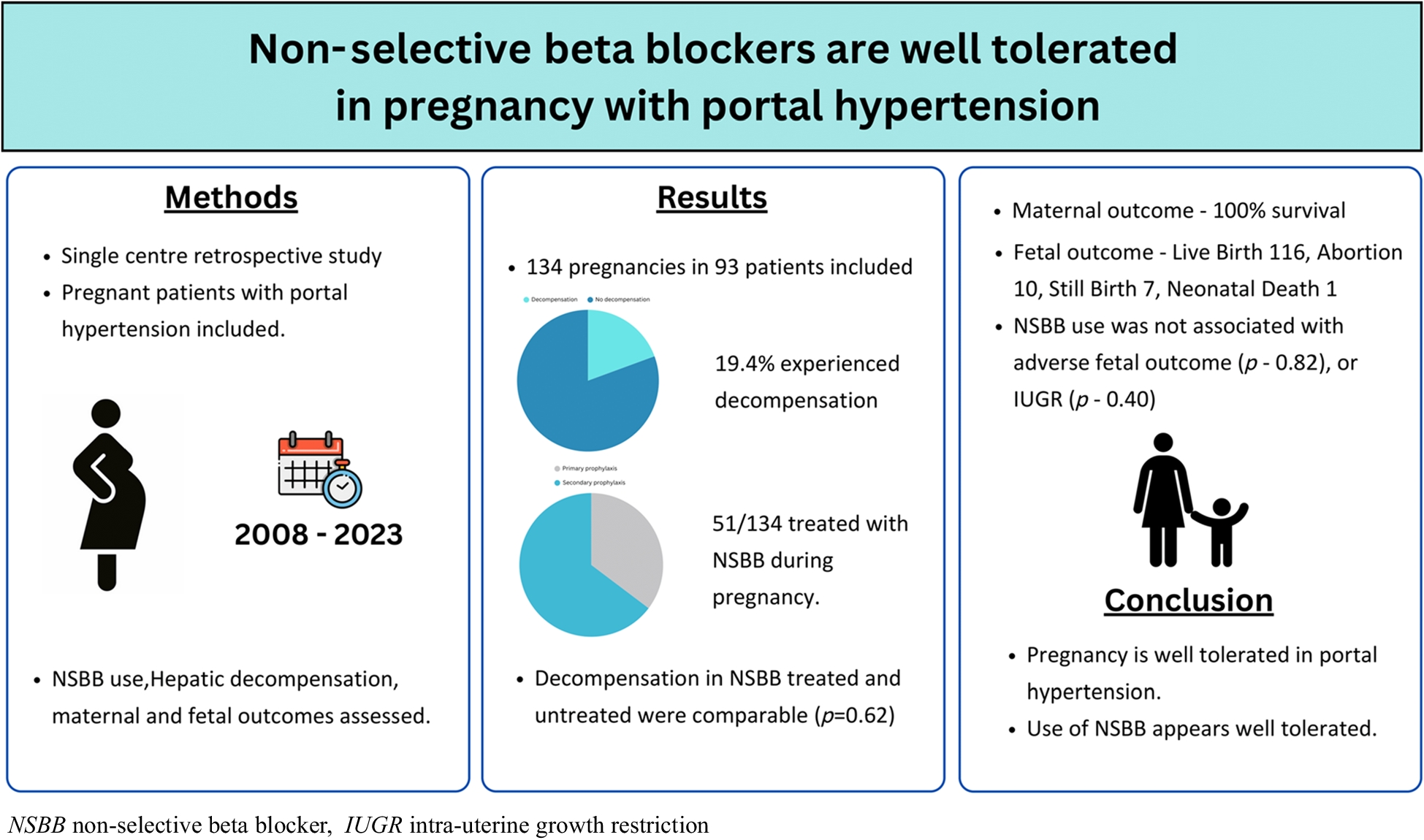
Fig. 6
Diagnostic algorithm for suspected mass in pancreas and differentiation from autoimmune pancreatitis. CECT contrast-enhanced computed tomography, MPD main pancreatic duct, AIP autoimmune pancreatitis, IgG4 immunoglobulin G4, CA 19-9 carbohydrate antigen 19-9, EUS endoscopic ultrasound, FNB fine needle biopsy
Therapeutic monitoringEUS can effectively visualize steroid-induced changes in the pancreatic parenchyma and ductal structures such as parenchymal hypertrophy, hyperechoic foci, hyperechoic strands, lobularity and a high-echoic margin of the main pancreatic duct. These features often respond to steroid therapy with atrophy seen after therapy (Fig. 5). Unlike abdominal ultrasound, EUS provides clearer imaging of these specific findings, offering a potential advantage in diagnosing and monitoring AIP [24, 55].
With the ongoing advancements in technology, the integration of artificial intelligence (AI) into EUS imaging holds great promise for enhancing diagnostic accuracy. Marya et al. [56] developed an EUS-based convolutional neural network (CNN) to differentiate AIP from PC, chronic pancreatitis (CP) and normal pancreas (NP). Trained on EUS images and videos from 583 patients, the model showed high sensitivity and specificity, including 99% sensitivity and 98% specificity for distinguishing AIP from NP and 90% sensitivity with 93% specificity for AIP vs. PC. This CNN model offers the potential for earlier, more accurate diagnosis of AIP, improving patient outcomes and management [56].
In summary, EUS has become an increasingly valuable tool in the diagnosis and management of AIP, offering detailed imaging and tissue acquisition capabilities. EUS remains an underutilized but pivotal modality in India for the early and accurate diagnosis of AIP. Emerging technologies such as EUS-based artificial neural networks, hold promise for enhancing diagnostic precision but require further validation. To improve consistency in clinical practice, incorporating EUS-specific criteria into existing AIP diagnostic guidelines is essential. Despite these advancements, India lacks multicentre prospective studies—particularly those evaluating the role of EUS in AIP. There is a clear need for collaborative national registries and research networks to generate high-quality, region-specific data and to develop standardized diagnostic algorithms suited to the Indian population.
Comments (0)