
Remember me



This section describes the fabrication of a prototype based on the theoretical design outlined previously and assesses its performance through experimental validation under simulated surgical conditions. A series of experimental methods were employed to empirically confirm the feasibility and technical reliability of the system.
Experimental environmentThe experimental setup, including the actual drill used, is shown in Fig. 5. The drill bit has a diameter of 2 mm, consistent with standard pilot drills used in clinical dental implant procedures. The central detection pin-responsible for identifying changes in bone quality-has a diameter of 0.6 mm and is designed to protrude 0.5 mm beyond the drill tip to ensure accurate detection. The axial movement of the detection pin is regulated by a compression spring with a spring constant of 14.024 N/mm and a maximum load of 18.93 N. This spring mechanism enables the pin to retract when encountering dense bone and to extend when contacting softer tissue. The drill is powered by a Maxon ECXSP13L BL KL A HP 24V motor, which provides precise rotational control essential for surgical applications.
Fig. 7
Positional response of the drill. Contact with the simulated bone occurred at 0.35 mm, with the automatic stop triggered at approximately 6 mm
Fig. 8
Force response during drilling with a 4 N load. A pressing force of approximately 4 N was maintained after the drill contacted the simulated bone
The experimental setup is illustrated in Fig. 6. In order to evaluate the functionality and reliability of the proposed dental implant drill, a custom-made pilot drill system was designed and tested in bench-top experiments.
A 5-mm-thick veneer board was employed as a bone analogue for the initial validation experiments. Veneer is constituted of a relatively hard surface layer and a softer inner layer, which enables partial reproduction of the difference in hardness between cortical and cancellous bone. According to Misch’s classification, the resistance of veneer corresponds to D2–D3 bone quality, thus making it a reasonable analogue for first-step validation of the detection mechanism. Despite the fact that veneer does not reproduce the porosity, hydration, or anisotropy of human bone, its use permitted a reproducible, low-cost, and controlled evaluation of the device.
The drill system has been engineered in such a manner that rotation commences exclusively upon the application of pressure to the detection pin, thereby ensuring the prevention of unintended activation. This is due to the fact that rotation becomes impossible outside the oral cavity. The drill was mounted on a controlled linear motion system that enabled perpendicular movement relative to the board surface, while continuously recording positional and force data.
The veneer bone surrogate was placed at a depth of 0.35 mm, after which drilling tests were conducted under two controlled loading conditions of 4 N and 5 N, applied in the axial direction. It is important to note that these force values represent cutting load conditions, as opposed to threshold forces. This enables an examination of the behaviour of the detection mechanism under realistic operational parameters. The system was programmed to automatically terminate the drill’s forward and backward motion if a penetration state persisted for more than 0.2 s. Each experimental condition was replicated 12 times. The data were analysed using descriptive statistics and t-tests to evaluate differences between conditions.
Experimental resultsFig. 9
Result of the penetration experiment. The automatic stop mechanism was activated immediately upon drill penetration of the simulated bone
Representative results are presented in Figs. 7 and 8. Figure 7 depicts the positional response of the drill along the linear motion axis, while Fig. 8 displays the corresponding force response. Figure 9 shows the veneer board following automatic drill cessation upon penetration detection, demonstrating the immediate stop after breakthrough.
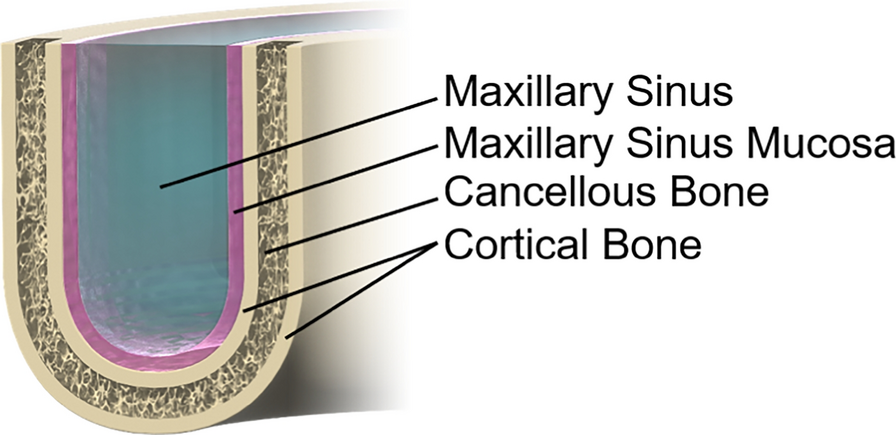
As outlined in Table 1, a comprehensive statistical analysis was conducted for both 4 N and 5 N loading conditions, as detailed in the table provided. In the 4 N condition, the mean residual bone thickness at the time of sensor activation was recorded as 0.47 mm (95 % CI 0.34\(-\)0.59). This finding suggests that the process was terminated prior to perforation, a consequence of the vibration-induced stress. This outcome is indicative of a safety-oriented conservative configuration. It is important to note that the typical physiological thickness of the maxillary sinus membrane is less than 1 mm, which provides a favourable safety margin. Conversely, under the 5 N condition, perforation occurred with consistent regularity, exhibiting an average overshoot of 0.85 mm (95 % CI 0.56\(-\)1.13) and a maximum of 1.7 mm. This setting, oriented towards efficiency, resulted in a substantial augmentation in perforation risk. A t-test was conducted, revealing a statistically significant difference between the two conditions (p = 0.027). This finding demonstrates the trade-off between safety and efficiency in the performance of the detection mechanism.
With regard to the reduction of time, the 5 N condition resulted in a statistically significant reduction of approximately 1 s in comparison with the 4 N condition (p = 0.012). Furthermore, the drill’s travel speed exhibited an approximate increase of 0.5 mm/s under the 5 N load, which proved to be statistically significant (p = \(5.52 \times 10^\)). This finding suggests enhanced efficiency and the possibility of reducing the overall duration of the surgical procedure. However, it is important to note that the 4 N condition demonstrated a lower risk of perforation, indicating superior safety performance.
The initial travel distance required for the detection pin to be fully depressed and trigger the drilling operation was approximately 0.2 mm under both loading conditions. No statistically significant difference was observed between the 4 N and 5 N cases (p = 0.077 > 0.050). This finding suggests that the activation distance is predominantly determined by the mechanical characteristics of the spring and the initial protrusion length of the detection pin, rather than by the applied cutting load.
The experimental results presented in this section confirm the fundamental effectiveness of the proposed medical drill equipped with a safety mechanism. The findings demonstrate the efficacy of the detection mechanism in reliably distinguishing transitions from harder to softer material, with overshoot values limited to less than 2 mm. The sensor is mounted directly on the drill tip, and it is subjected to constant pressing force during cutting. As a result, mechanical play or backlash in the drive system does not influence detection accuracy. Therefore, the overshoot values reported in this study are indicative of the system’s actual limits. However, the findings also highlight the need for further system optimisation and more comprehensive clinical validation. It is recommended that future research involve testing under a wider range of loading conditions, the use of diverse biological tissue analogues, and evaluation within actual physiological environments.
Table 1 Summary of drill performance under cutting loads of 4 N and 5 N
Comments (0)