
Remember me


We evaluated the changes in regional cerebral tissue saturation of 126 patients who underwent elective carotid endarterectomy at Városmajor Heart and Vascular Center, Semmelweis University, Budapest, between 2019 and 2021 (May 13, 2019–Nov 04, 2021). After providing full information, all the patients gave written consent to participate in the study according to the guidelines approved by the Ethical Committee of Semmelweis University (Semmelweis University Regional and Institutional Committee of Science and Research Ethics, 17/2019, 02/15/2019). The study was performed according to the Declaration of Helsinki, and it was registered on ClinicalTrials.gov (NCT03907943) on Mar 26, 2019.
The indication for endarterectomy was carotid artery stenosis, with stenosis exceeding 70% based on the NASCET (The North American Symptomatic Carotid Endarterectomy Trial) criteria [15]. All of our patients were asymptomatic.
The exclusion criteria were lack of consent, history of dementia, symptomatic carotid artery stenosis, and atrial fibrillation. An MMSE score below 24 points was a contraindication for enrollment, and those who were not able to reach this value were not tested further. The Cronbach’s alpha of our population regarding their MMSE scores was 0.79.
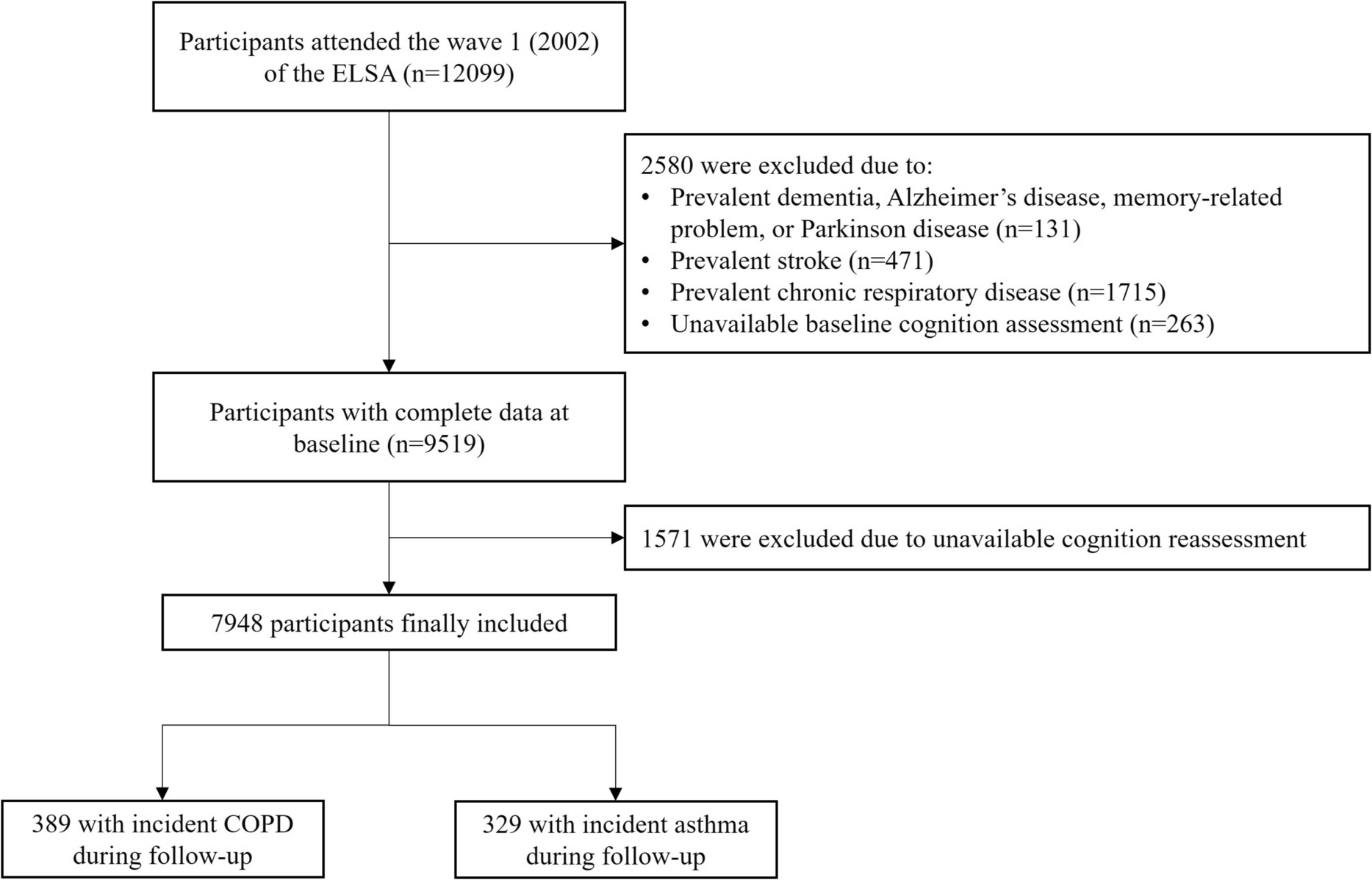
The flow diagram of the enrollment and follow-up is shown in Fig. 1. From May 2019 to November 2021, we enrolled 129 patients. All patients completed the MMSE and the MoCA preoperatively. Three patients were excluded due to the presence of cognitive impairment in the preoperative MMSE. In 115 cases, we have the proper record of the anesthesiological monitoring.
Fig. 1
Consort flow diagram of the enrollment and follow-up
Three-month postoperative cognitive assessments were completed in 103 patients. One patient died before the first control (SARS-COVID pneumonia), and 11 patients did not return to our follow-up visit.
The decision about the type of surgery and the indication for shunt use was made by the surgeons based on the patients’ anatomy of the circle of Willis, the condition of the contralateral internal carotid artery (ICA), and the position of the stenosis. The anatomy of the circle of Willis was analyzed and classified as complete (no component was absent or hypoplastic) or incomplete.
All patients underwent balanced general anesthesia. Anesthesia was induced with propofol (2–5 mg/kg or until loss of consciousness) and fentanyl (2–10 mcg/kg). For maintenance, we used sevoflurane (114 patients, 1,8–2 MAC) or isoflurane (12 patients, 1,2–1,4 MAC) and fentanyl (0,02 mg/kg—or as necessary to avoid signs of pain) as analgesic agents. For muscle relaxation, atracurium or rocuronium was used. The choice of the volatile agent and the muscle relaxant was at the discretion of the anesthesiologist. After intubation, all patients were ventilated with 40–50% oxygen, aiming to maintain end-tidal carbon dioxide between 33 and 40 mmHg.
The anesthesia station was a GE Aisys CS2. Routine monitoring included electrocardiogram, intra-arterial blood pressure measurement, pulse oximetry, capnography, and entropy. For sufficient depth of anesthesia, state and response entropy values were maintained between 40 and 60 [16]. Before clamping, 2500 IU of heparin was administered to all patients. At the end of the procedure, heparin was reversed with protamine.
Bilateral frontoparietal regional cerebral tissue oxygenation (rSo2) was measured using a Somanetics Invos™ 5100C cerebral oximeter. NIRS monitoring was started after arrival to the operating room, continued throughout the whole procedure, and finished just before the patients left the operating room. The sampling frequency was 0.166 Hz. The phases of the operation were accurately marked in all the monitors.
As a baseline value, we determined the median of regional cerebral tissue saturation values of the 2-min-long preclamping (CCA clamping) period.
To prevent the evaluation of measurement errors, which would be misleading, we analyzed not one single value, but we looked for the serial of the lowest values lasting 30 second during the cross-clamp period. For further calculation, we used their median. So, the lowest cross-clamp saturation value was calculated from the median of the lowest saturation values lasting at least 30 second during the cross-clamp period (from clamping the CCA and ICA to the complete removal of the clamp). From these data, we calculated the ratio from baseline to the lowest cross-clamp values as a percentage using the following formula: (rSO2preclamp − rSO2clamp)/rSO2preclamp × 100.
The target mean arterial pressure ranged ± 20% of the preoperative level. In cases of hypotension, we used intravenous norepinephrine (0.01–0.1 mcg/kg/min) to maintain the mean arterial pressure at an adequate level, in the targeted range. Those patients who showed bradycardia tendency during vessel preparation received lidocaine infiltration of the surgical area.
Neuropsychological testsPatients’ cognitive evaluation for general cognitive impairment detection included the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) supervised by the same physician (SA- HU710556625-01).
Neurocognitive testing was performed preoperatively, a day before surgery, and the next survey was scheduled at 3 months after the surgery.
Our survey contained elements to assess patients’ condition with regard to frailty. We had questions aiming to obtain a picture of their medical history, general condition, social situation, level of education and profession, capability of self-care, and, superficially, their psychological condition and history.
Cognitive evaluation started with the MMSE to exclude those suffering from dementia. The cutoff value for the MMSE was 24 points, and those who were not able to reach this value were not tested anymore [17]. The survey continued with a discussion about the frailty parameters and was closed completing the MoCA test. The 8.1 version of the MoCA test was used. Changing the version of the MoCA test made it possible to eliminate the risk of the learning effect.
A decrease in the test scores with a minimum of the standard deviation of the results of the preoperative test or more (MMSE: 1.79, MoCA: 2.28) was considered a cognitive decline (PNCD) and an increase with the same amount as cognitive improvement (POCI) [18].
Statistical analysisAll statistical analyses were performed using SPSS software (IBM SPSS Statistics Version 20). A P value < 0.05 was considered statistically significant. To analyze the distribution of the data, we used the Kolmogorov‒Smirnov test. Normally distributed data are presented as the mean and standard deviation, and non-normally distributed data are presented as the median and interquartile range. Categorical variables are presented as numbers and percentages. For comparing groups, we used the Mann‒Whitney U test in the case of non-normally distributed data and Student’s t test for normally distributed data. Discrete data were compared using Pearson’s chi-squared test.
To compare the differences among patients with different directions of cognitive change (three groups), we used univariate analysis of variance in cases of normally distributed data, the Kruskal‒Wallis test in cases of non-normally distributed data, and Pearson’s chi-squared test for categorical data. As a post hoc test, we applied the Mann‒Whitney U test.
We performed univariate logistic regression analysis for all variables to predict PNCD and POCI. With the multivariable logistic model, we analyzed factors with a p value less than or equal to 0.15.
The correlation between the rSO2 values, the degree of desaturation during the clamping period, and the change in the scores of the cognitive test were evaluated with Spearman’s correlation analysis.
The best cutoff of rSO2 decrease for the detection of intraoperative hypoperfusion causing changes in cognitive performance was analyzed by receiver operating characteristic (ROC) curves. SPSS software (IBM SPSS Statistics Version 20) was used to create figures.
Comments (0)