The primary objective of this study was to identify immune subtypes of CHOL through a comprehensive analysis of transcriptome and single-cell sequencing data and to explore their implications in the metabolic regulation of macrophage functions in inflammation [28]. We successfully identified two distinct immune subtypes: immune-infiltrated (CS1) and immune-depleted (CS2). CS1 exhibited a highly active TME with substantial immune cell infiltration and activation of immune-related signaling pathways, whereas CS2 was characterized by a deficiency in immune components and a poorer prognosis. Furthermore, we discovered that the downregulation of oxidative phosphorylation in macrophages within CS1 likely drives a shift towards glycolysis, enhancing their activation state. These findings provide valuable insights into immune subtype classification, biomarker identification, and the development of targeted immunotherapies for CHOL.
The limited efficacy of surgical resection has contributed to the unsatisfactory prognosis of CHOL [6, 7]. Consequently, precision medicine has emerged as a promising approach for developing personalized therapies based on molecular subtypes, and has been extensively studied in various cancer types. Previous studies have explored potential immune subtypes in CHOL and examined their response to immunotherapy [29,30,31]. However, these studies relied on immune gene expression profiles to classify immune subtypes in CHOL. Job et al. previously classified CHOL into four immune subtypes based on immune-infiltrating cells [32], but their study solely focused on intrahepatic CHOL and did not consider perihilar and distal CHOL. As such, our current study represents the first attempt to identify immune subtypes in CHOL by analyzing the enrichment scores of immune-infiltrating cells within the TME.
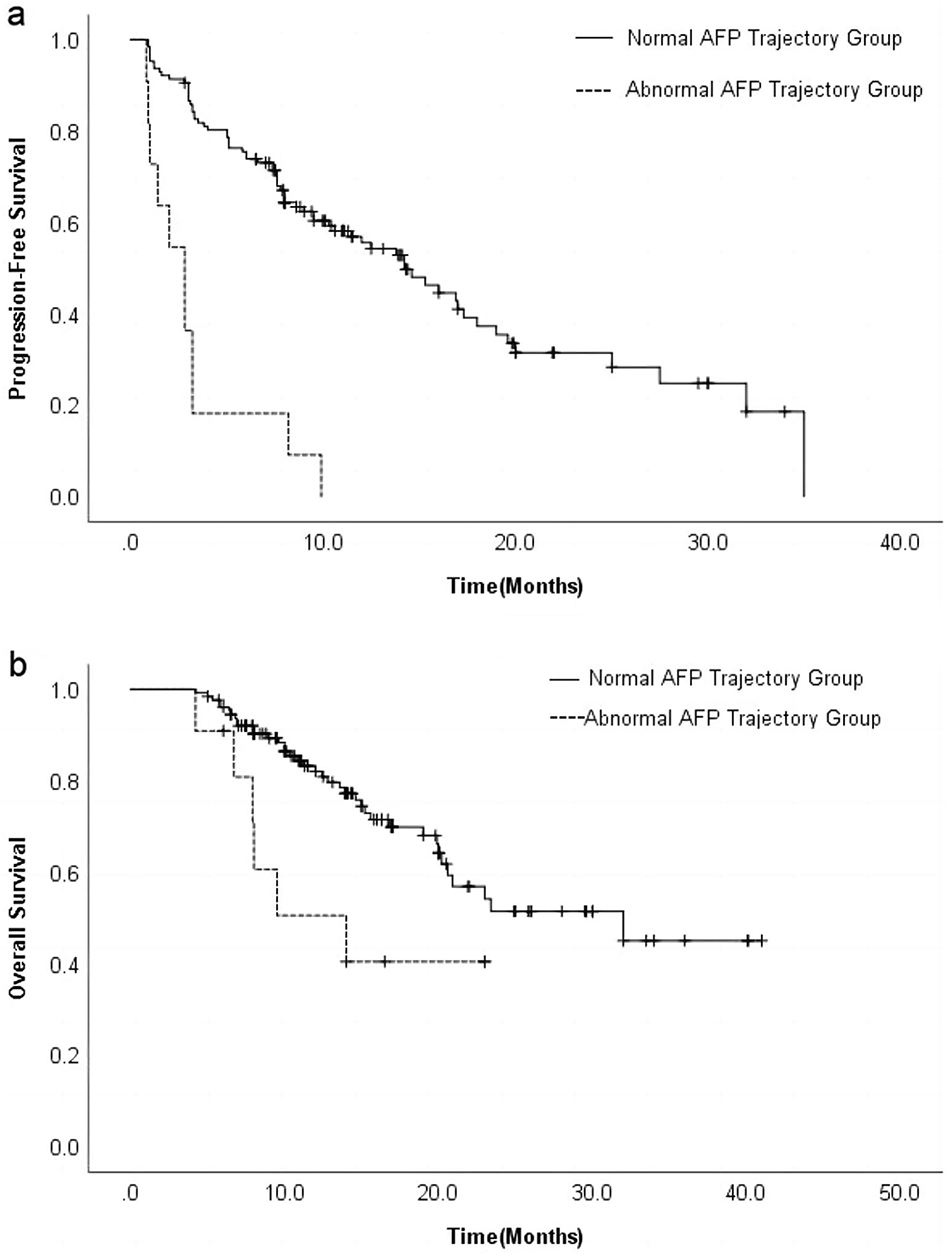
The present study has successfully characterized immune-infiltrated CS1 and immune-depleted CS2 subtypes in CHOL, based on the infiltration levels of ten distinct immune cell types. Our analysis revealed that CS1 exhibited a pronounced immune landscape within the TME, characterized by higher levels of immune cell abundance, enhanced immune regulatory activity, elevated expression of immune checkpoint markers, and increased IES and SES scores. Conversely, CS2 was typified by an immune-cold profile, with limited immune cell infiltration and attenuated immune activity. Importantly, our analysis demonstrated that patients belonging to the CS1 subtype exhibited a significant improvement in progression-free survival (PFS) compared to those in CS2. These findings align with previous studies, which have similarly reported that CHOL subtypes with an active immune landscape are associated with favorable clinical outcomes. Our GSEA functional enrichment analysis further revealed that several immune-related signaling pathways were significantly upregulated in the immune-infiltrated CS1 subtype. Concurrently, the oxidative phosphorylation process, which plays a critical role in tumorigenesis and tumor progression, was markedly attenuated in this subtype. The findings of Raggi et al. corroborate our results [33], which indicate that CHOL patients with heightened mitochondrial oxidative metabolism exhibit poorer prognosis. Conversely, our analysis suggests that patients belonging to the CS1 subtype, characterized by weakened oxidative phosphorylation, may experience a more favorable clinical outcome. CTLA4, PD1, and PDL1 are the major immune checkpoints in the TME, and their strong expression levels have been shown to suppress immune responses and limit the efficacy of immunotherapy [34]. In line with our study, previous research has also demonstrated that CHOL subtypes characterized by an inflamed TME may be more responsive to immunotherapy.
Our study has demonstrated the existence of two distinct immune subtypes in CHOL, characterized by immune-infiltrated CS1 and immune-cold CS2, with this classification independently validated using external cohorts. These subtypes likely play a critical mechanistic role in the generation and progression of CHOL. In the immune-infiltrated CS1 subtype, the presence of activated immune cells, particularly macrophages and T cells, within the tumor microenvironment suggests an enhanced anti-tumor immune response. Macrophages in CS1 appear to undergo metabolic reprogramming, shifting towards glycolysis, which supports their pro-inflammatory and tumoricidal functions. Conversely, the immune-cold CS2 subtype, characterized by a deficiency in immune cell infiltration and activation, may contribute to an immunosuppressive tumor environment, allowing tumor cells to evade immune surveillance and promoting tumor progression. These findings provide compelling evidence of the clinical relevance of these subtypes, strongly suggesting that patients in the CS1 subtype may benefit from immunotherapy. Future analyses could investigate the prognostic impact of immune activators and suppressants in both subtypes and explore the activation or inhibition of different signaling pathways.
The critical role of epigenetic regulation of DNA enhancer methylation in shaping the heterogeneity between cancer subtypes has been extensively documented [30, 35,36,37]. Our analysis revealed that epigenetic alterations play a crucial role in defining specific cellular phenotypes in CS1, characterized by activated immune regulatory pathways and silenced oxidative phosphorylation. These observations are in line with our results from GSEA functional enrichment analysis, further emphasizing the importance of epigenetic regulation in shaping the molecular landscape of CHOL subtypes. Our study highlights the crucial role of epigenetic regulation of DNA methylation in driving TME remodeling and regulating energetic metabolism in CHOL. Our results suggest that transforming the immune-cold subtype into an immune-infiltrated subtype at the epigenetic level may represent a promising therapeutic strategy for improving clinical outcomes in CHOL [38].
Genome instability, as characterized by the fraction genome altered, has been shown to be associated with dysfunction of DNA repair mechanisms, which is strongly correlated with more advanced stages of cancer progression [39]. Consistent with previous research, our study revealed that the CS2 subtype, which was associated with poorer prognosis, exhibited higher levels of genome instability. We observed that CNVs, a type of structural variation in the genome, were a key contributor to this instability, which can result in abnormal gene copy numbers and subsequently promote cancer onset and progression [40]. Previous studies have reported that depletion of chromosome 4 due to CNVs is associated with the formation of an immune-cold TME [24]. Consistent with these previous findings, we observed a depletion of chromosome 4q35.2 in the CS2 subtype, which likely contributed to the development of a silenced immune landscape in this subtype. Intriguingly, we found that the two pivotal immune regulatory genes, LRBA and NF-κB1, were mapped to nearby regions on chromosome 4q31.1 and 4q24, respectively, which suggests a potential mechanism by which the observed depletion at chr4q35.2 may impact immune regulatory processes in CHOL. Our correlation analysis further supported this observation, as we found a significant positive correlation between the depletion at chr4 and the low expression levels of LRBA and NF-κB in the CS2 subtype. This suggests that the observed depletion at chr4q35.2 may impact the transcription of contiguous genes, particularly LRBA and NF-κB1, ultimately contributing to the development of an immune-cold phenotype in this subtype. IDH1 mutations are commonly found in cholangiocarcinoma, with a prevalence ranging from 9 to 13% [41]. In our study, we observed that IDH1 mutations were more prevalent in the CS2 subtype, while multiple gene mutations were equally detected in the CS1 subtype. These findings suggest that there may be a distinct mutation landscape underlying the different CHOL subtypes. However, further investigation with larger cohorts is needed to validate and expand upon these initial observations.
Our study demonstrated that the immune-cold CS2 subtype is a significant risk factor for both OS and PFS in CHOL patients. The high hazard ratios associated with the CS2 subtype underscore the importance of timely and comprehensive evaluation and treatment for patients with this subtype, and may serve as a valuable tool for clinicians in predicting clinical outcomes and guiding treatment decisions for CHOL patients. Furthermore, our study identified sunitinib and X681640 as potentially sensitive chemotherapy agents for the immune-infiltrated CS1 subtype of CHOL.
DLX5 has been identified as a driver of cancer progression in a variety of cancer types [42,43,44]. However, the potential role of DLX5 in CHOL has not yet been explored. In our study, we provide experimental evidence demonstrating that knockdown of DLX5 leads to attenuated proliferation and migration capabilities of CHOL cells. These findings provide a strong foundation for further research aimed at elucidating the potential role of DLX5 in CHOL progression and identifying DLX5 as a potential therapeutic target for this disease.



Comments (0)