Recently, combination therapies have become the standard treatment for advanced HCC [11]. AFP is a widely recognized biomarker for HCC diagnosis, monitoring, and prognosis, with changes in AFP levels closely correlated with treatment outcomes and prognosis [12]. However, an unusual phenomenon was observed during advanced HCC treatment, particularly in patients receiving combination regimens that include targeted immunotherapy. In these cases, AFP levels decreased despite continued HCC progression. Previous studies have noted that in the progressive disease (PD) subgroup, patients treated with ramucirumab had a significantly lower rise in AFP from baseline compared with those treated with placebo [13]. This suggests that despite disease progression, elevated AFP levels can be suppressed in some patients, and AFP may even decline. Here, for the first time, we analyse this phenomenon in detail.
In clinical practice, immune checkpoint inhibitors occasionally lead to tumor enlargement or new lesion formation, followed by subsequent tumor reduction or resolution, a phenomenon known as pseudoprogression [14]. This is believed to result from immune cell infiltration, tumor necrosis, hemorrhage, and lesion edema [15]. Pseudoprogression is primarily identified through imaging follow-up, with clinical trials reporting its incidence in melanoma (4.6–8.3%), non-small cell lung cancer (1.8–6.9%), and renal cell carcinoma (4.9–7.1%). In HCC, however, pseudoprogression is rare [16,17,18]. Herein, the observed abnormal AFP trajectory phenomenon in patients with HCC—characterized by AFP reduction concurrent with HCC progression—represents true progression rather than pseudoprogression. This is confirmed by continued imaging-documented tumor growth and later re-elevation of AFP levels alongside disease progression.
Among the 11 patients with abnormal AFP trajectories, nine were treated with targeted immunotherapy as part of their regimen. These abnormalities occurred either at therapy initiation or during treatment, with six patients exhibiting abnormalities early and five developing them later. The median duration of this phenomenon was 63 (range: 36–97) days, with two patients still demonstrating abnormal trajectories at the end of follow-up. For the remaining nine patients, AFP changes coincided with synchronous imaging evidence of tumor progression. This suggests that abnormal AFP trajectories occur at specific treatment stages rather than consistently throughout the disease course. These phenomena may be transient, making them difficult to detect without regular monitoring.
In this cohort of 139 patients with advanced HCC receiving systemic and/or local treatments, 11 patients (7.9%) exhibited abnormal AFP trajectories, indicating a relatively low incidence. This phenomenon may have been underreported in the past due to its transient nature and potential for being overlooked. However, in this study, the inclusion of regular follow-ups at 1–2-month intervals facilitated the identification of such abnormalities. These abnormal AFP trajectory phenomena reduce the reliability of AFP as a standalone marker for evaluating treatment efficacy and prognosis.
To improve detection and accurate assessment of tumor progression in patients with advanced HCC, dynamic analysis of AFP levels must be integrated with imaging studies. This combined approach is critical for identifying tumor progression and optimizing patient management strategies.
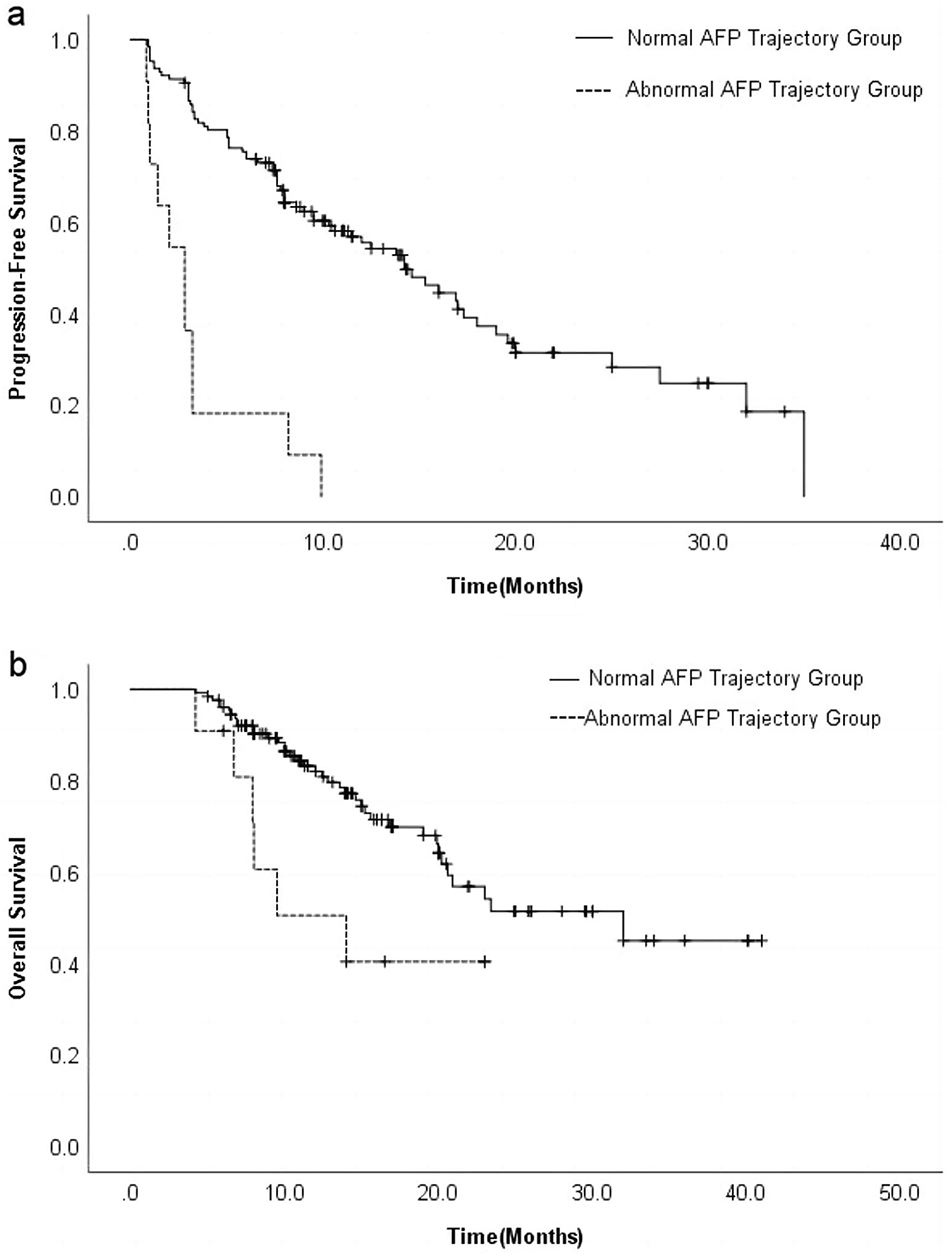
Of the 11 patients exhibiting abnormal AFP trajectories, eight altered their treatment plans following the onset of this phenomenon. Among these, seven patients transitioned to triple therapy involving TACE and targeted immunotherapy, accompanied by multiple adjustments in targeted drugs; however, disease progression persisted. In contrast, one patient achieved stable disease following radiofrequency ablation for newly developed small lesions. The ORR and DCR of the AFP abnormal trajectory group were significantly lower than those of the AFP normal trajectory group at 3 months post-treatment. Additionally, the mPFS and mOS were significantly shorter, underscoring the association of abnormal AFP trajectories with poor treatment efficacy, rapid disease progression, potential drug resistance, and an overall unfavorable prognosis. This phenomenon highlights the necessity of close clinical monitoring.
Notably, nine out of 11 patients with abnormal AFP trajectories were receiving targeted immunotherapy when the abnormal trajectory emerged. Multivariate logistic regression analysis identified combined targeted immunotherapy as an independent risk factor for this phenomenon, with an OR of 15.35, indicating a strong association. Beyond its role as a molecular marker, AFP plays a critical role in HCC pathogenesis and progression. Specifically, AFP contributes to tumorigenesis by inhibiting the p53/Bax/caspase-3 apoptosis pathway, inducing the malignant transformation of hepatocytes, promoting tumor invasion and angiogenesis, and suppressing immune cell function. These processes collectively enable HCC cells to evade immune surveillance, survive, and metastasize [19, 20].
Therefore, it is speculated that during advanced HCC treatment—particularly with targeted immunotherapy—tumor cells may actively downregulate AFP expression as a mechanism to evade AFP-targeted immune responses. This abnormal trajectory phenomenon could represent a form of tumor immune evasion and self-protection, accompanied by the development of drug resistance. Further research is required to elucidate the precise molecular mechanisms underlying this phenomenon, which may provide new insights into overcoming treatment resistance in advanced HCC.
Neutrophils play a significant role in cancer progression by enhancing angiogenesis, promoting tumor cell proliferation and metastasis, and facilitating immune evasion [21]. A reduction in the proportion of lymphocytes suggests a weakened cell-mediated immune response to cancer [22]. Research indicates that neutrophils may undergo immunosuppressive changes in cancer, particularly in their interactions with T cells. Strategies to inhibit neutrophil mobilization and recruitment into tumors may enhance the efficacy of cancer immunotherapy. A low NLR has been identified as an important predictor of pembrolizumab efficacy [23], whereas a high NLR is recognized in clinical practice as an independent prognostic indicator of poor cancer outcomes and a marker of systemic inflammation [24, 25].
In the context of HCC, studies reveal that an elevated baseline NLR is associated with worse survival outcomes. For instance, among patients receiving TACE as first-line therapy for stage B HCC, a baseline NLR of ≥ 3 was linked to disease progression within 6 months. Similarly, in a cohort of 380 patients with newly diagnosed HCC undergoing TACE, those with a normal baseline NLR (≤ 2.4) had a mOS of 29.1 months, compared to 19.1 months [26] for those with an elevated NLR (> 2.4).
Herein, the baseline NLR in the AFP normal and abnormal trajectory groups was 2.54 and 3.98, respectively. The ORR, DCR, PFS, and OS were significantly lower in the AFP abnormal trajectory group. These findings indicate that patients in this group experienced poorer treatment efficacy and faster disease progression. Consequently, the baseline NLR should be considered a prognostic factor in HCC. High baseline NLR was also identified as an independent risk factor for the AFP abnormal trajectory phenomenon, which is consistent with previous studies linking NLR to immune escape mechanisms.
This study has several limitations. As a retrospective analysis, potential confounding factors may have influenced the results. Between March 2021 and May 2023, 139 patients were recruited. The abnormal trajectory phenomenon was detected in 11 hepatitis B - positive cases only. This likely stems from hepatitis B being the leading cause of HCC in China. Given the small sample size, the phenomenon might occur in non - viral HCC cohorts but was not observed in our study. Moreover, the small sample size of the abnormal - trajectory group and its internal heterogeneity may have undermined the study’s conclusions, underscoring the necessity for large - scale prospective clinical validation.
In conclusion, a subset of patients with advanced HCC exhibit abnormal AFP trajectories during treatment. This phenomenon is associated with HCC progression, resistance to current targeted immunotherapy, and poor prognosis. Modifying targeted immunotherapy regimens in these patients may not improve outcomes. Combined targeted immunotherapy and elevated baseline NLR are independent risk factors for the development of this phenomenon. Clinically, patients exhibiting these risk factors require close monitoring to optimize management strategies. In the future, it is necessary to conduct relevant experiments to clarify the mechanism by which AFP participates in immune escape during HCC treatment, so as to explore related treatment options.



Comments (0)