One of the most severe complications following pancreatoduodenectomy (PD) is postoperative pancreatic fistula, which occurs in up to 3–45% of cases [15,16,17]. This complication is linked to 70% of sepsis and hemorrhagic events, leading to extended hospital stays and increased treatment costs. It poses a potentially life-threatening risk to patients, highlighting the importance of early prediction and perioperative management of these complications [18, 19]. The prevention and management of pancreatic fistula pose a significant therapeutic challenge for surgeons.Previously identified predictors of POPF encompass surgical factors such as the softness of the pancreas, a narrow pancreatic duct diameter, the duration of the operation, and intraoperative bleeding, as well as patient-related factors such as obesity, preoperative malnutrition, levels of amylase and calcitoninogen, C-reactive protein levels, sarcopenia, and albumin levels [18,19,20,21].
The primary aim of this study was to assess the prognostic importance of preoperative abdominal fat thickness as observed on CT scans.In the present study, multivariate logistic regression analysis identified the AFT as a significant independent prognostic factor for POPF in patients with pancreatic cancer following PD. The combined model’s superior specificity (81.4% vs. 52%) addresses a critical limitation of standalone imaging biomarkers by reducing false-positive predictions, thereby avoiding unnecessary interventions in low-risk patients.This enhancement reflects the complementary biological mechanisms captured by the model: AFT quantifies localized mechanical stress at the pancreaticojejunal anastomosis [22,23], soft pancreatic texture indicates parenchymal fragility prone to enzymatic leakage [3], and elevated TAG levels correlate with systemic inflammation that exacerbates tissue healing impairment [28].Clinically, this model could guide selective use of prophylactic measures.From a nutritional standpoint, visceral obesity is considered a crucial aspect of metabolic syndrome, which is associated with pro-inflammatory cytokines, chronic inflammation, and insulin resistance. These factors may lead to postoperative complications [24]. Recent research has investigated the relationship between body composition and postoperative outcomes in patients with PD. These studies have revealed that muscle mass and fat components are linked to the prognosis of PD, highlighting the significance of preoperative interventions aimed at improving body composition [25, 26].Several studies have indicated a correlation between sarcopenia and postoperative complications [27]. However, in our study, sarcopenia alone was not significantly associated with POPF, potentially due to the high proportion of elderly participants in our sample.The correlation between intra-abdominal adiposity and the occurrence of postoperative pancreatic fistula is often attributed to several factors. Excess adipose tissue can hinder surgical recovery by releasing cytokines, such as leptin, TNF-α, interleukin-1, and interleukin-6, which promote local inflammatory responses. Furthermore, adipose tissue has an immunosuppressive effect, which not only accelerates the development of pancreatic fistula but also further suppresses the immune system and delays wound healing. Additionally, the presence of adipose tissue surrounding the pancreas, coupled with the narrow diameter of the pancreatic duct, complicates the anastomosis process and reduces the local blood flow required for optimal healing [28, 29].
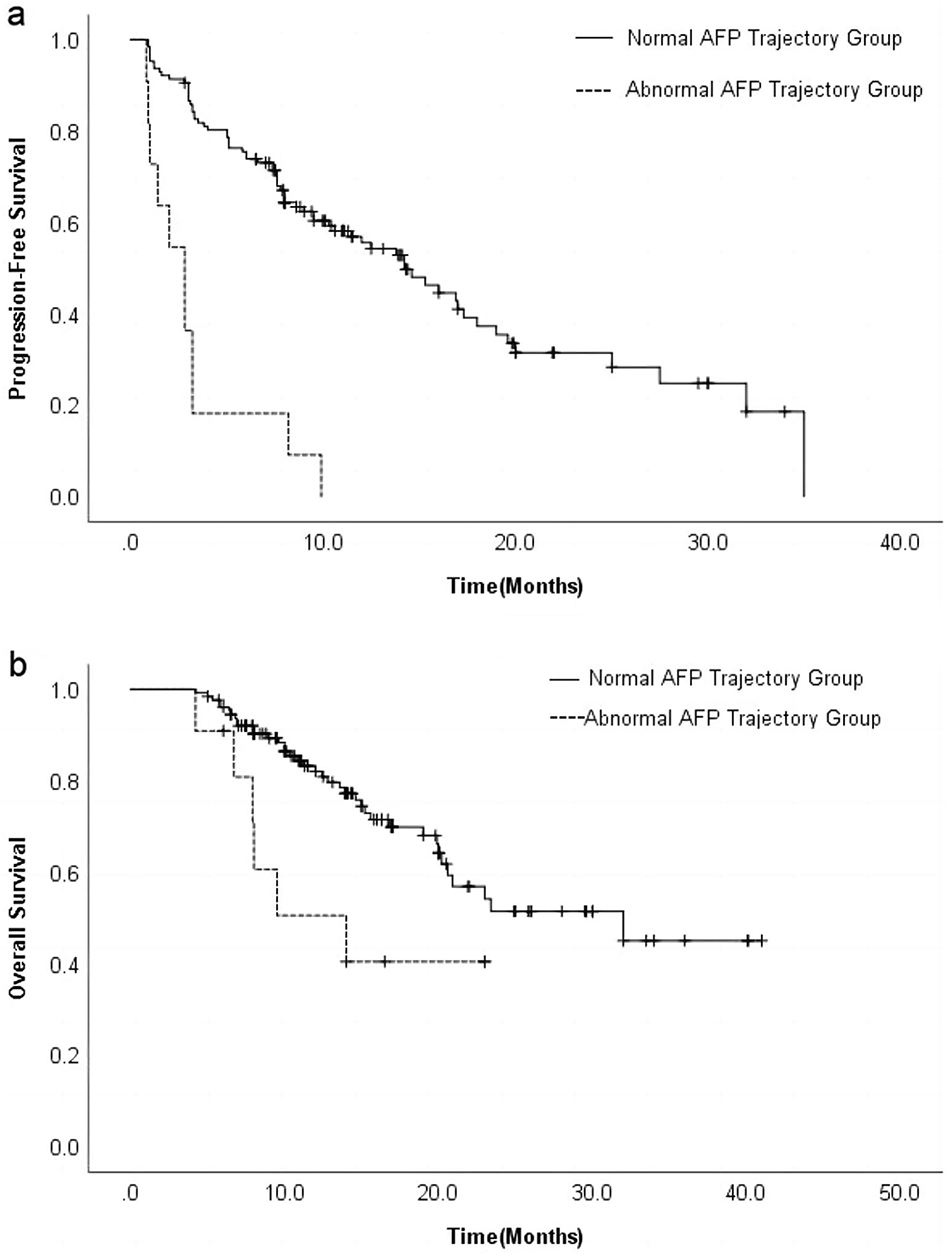
Furthermore, we also evaluated the role of AFT in predicting the prognosis of patients with PDAC following surgical resection. Our findings indicated that a high level of AFT served as a reliable indicator of a poor prognosis.Our study found that the AFT serves as an independent predictor of both overall survival (OS) and recurrence-free survival (RFS) in patients undergoing PD. Notably, patients with high AFT levels exhibited significantly lower OS and RFS compared to those with low AFT levels.Numerous studies have established significant associations between body composition parameters and pancreatic cancer prognosis, particularly focusing on sarcopenia, visceral adiposity, and their clinical implications. Sarcopenia, characterized by reduced skeletal muscle mass, has been consistently identified as an independent predictor of poor overall survival (OS) and postoperative complications in resectable PDAC [30,31,32]. Given that patients with pancreatic cancer require regular hospital visits for chemotherapy or targeted therapy following surgery, we excluded patients who did not undergo regular chemotherapy to eliminate the potential influence of chemotherapeutic agents on postoperative OS and RFS in our analysis. An excessive amount of visceral fat enhances the distribution volume of drugs by promoting their accumulation in adipose tissue. Furthermore, it modifies the pharmacokinetics of chemotherapeutic agents by affecting hepatic and renal drug clearance, ultimately leading to reduced efficacy and heightened toxicity of these agents [33]. These factors could indirectly affect survival rates and PFS after pancreatic cancer surgery.
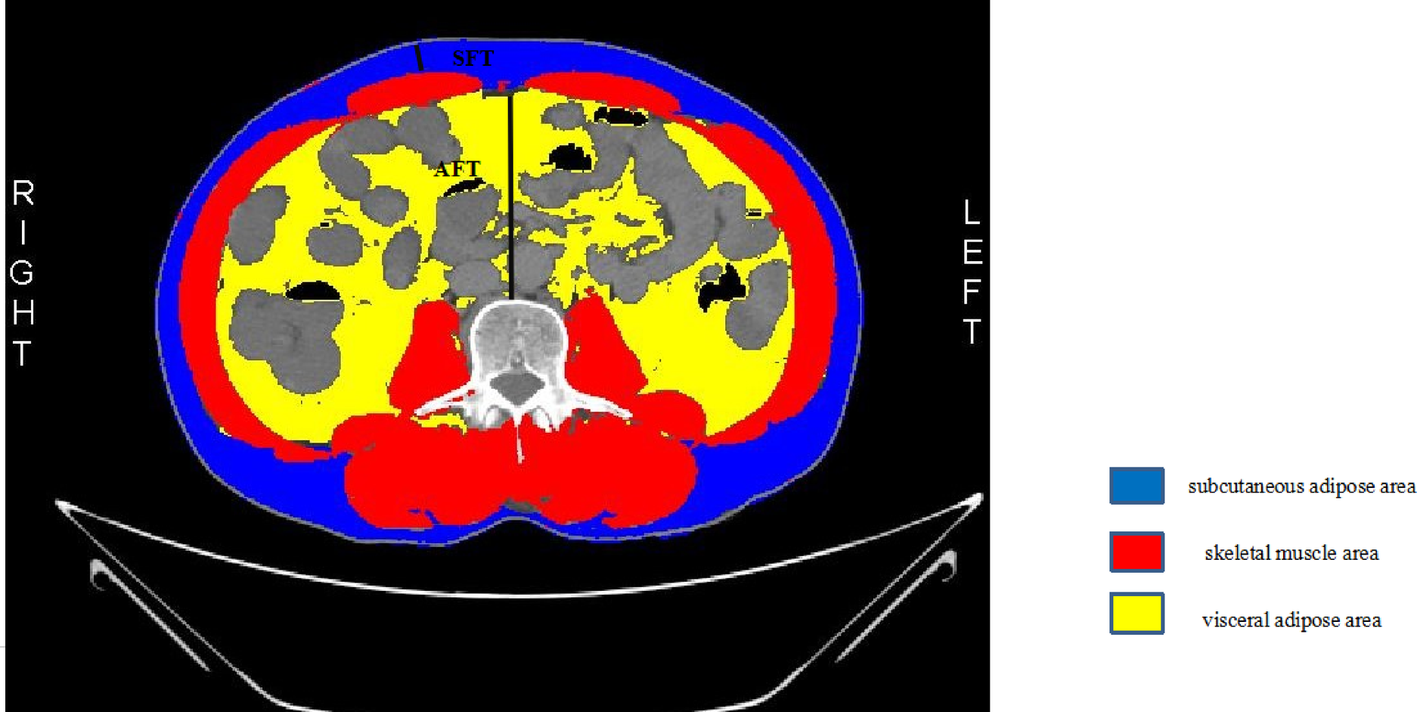
Body composition and perioperative serological indices are more readily available, and by assessing the area and thickness of visceral fat in patients, in conjunction with serum and body fluid composition, an adequate understanding of the patients’ risk of postoperative complications of pancreatic fistula may be achieved.However, it’s important to note that the relationship between intra-abdominal fat thickness and survival outcomes is likely to be influenced by a multitude of factors, including the stage of the cancer, the surgical technique employed, the patient’s overall health status, and the effectiveness of adjuvant therapies such as chemotherapy and radiation.It should be noted that this study is subject to certain limitations.Firstly, this was a retrospective study conducted at a single institution involving a relatively limited number of patients, and therefore the cut-off values calculated may not be entirely representative of other cohorts or hospitals. The cutoff values for preoperative AFT and serum indicators levels need to be validated through a prospective study.Meanwhile, we retrospectively collected data without any prospective component, which may potentially lead to issues in multivariable analyses due to the risk of incorporating similar factors.Secondly, the article was designed as a retrospective study, which may have introduced some selection bias. This requires further confirmation through prospective studies with larger samples.



Comments (0)