RAS mutation was present in almost half of indeterminate nodules, a finding that confirms the existing evidence [9, 14, 29]. Moreover, as already reported in several studies [7, 24, 30], the nodules were mainly distributed in the low and indeterminate categories of TIRADSs, and only about one out of 10 nodules was sonographically high suspicion. In agreement with the expected figures in TIRADSs [1, 24,25,26], MRs were higher in sonographically high suspicion nodules compared to sonographically low and intermediate suspicion nodules. However, in TIR3 nodules we found 100% of MR in sonographically very low suspicion nodules. These were four high risk (TIR3B) indeterminate nodules that were categorized as very low suspicion nodules according to the four TIRADSs but with malignant histology (two minimally invasive FTC and two tall cell subtype of PTC). This was moreover not surprising, since we know that TIRADSs perform suboptimally in FTC and the non-classical subtype of PTC [5, 6]. NRAS was the most common RAS mutation as it was detected in about two out of three RAS + nodules, this being in line with the current literature [14, 15, 20]. However, we did not find differences in MRs across the three isoforms of RAS, contrary to what other studies have reported (i.e., decreasing rates of malignancy from HRAS to NRAS to KRAS) [9, 31, 32]. As regards the histology of the 56 malignant cases, almost 50% were PTCs, the other 50% were equally distributed in NIFTPs and FTCs, and other 2 cases were WDT-UMPs. Specifically, among the 30 RAS + malignant cases (the remaining 28 RAS + cases were benign) there were eight classic PTCs, six fv PTCs, and eight NIFTPs, so that more than seven out of ten cases were potentially not aggressive thyroid cancers. The latter finding was already reported in other studies, according to which malignancy of RAS mutation alone is most likely associated with limited aggressiveness of thyroid cancer [31, 33]. In no case we did detect more than one mutation beyond that in RAS genes, and we included only BRAFV600E mutation–negative nodules.
In the present series, the accuracy of RAS testing was moderate irrespective of cytology (58% in cytologically indeterminate and 50% in suspicious for malignancy thyroid nodules). We found that RAS mutations had both specificity and PPV of 100% in cytologically suspicious for malignancy thyroid nodules, where MR was 91.7%. However, low values of SE (45.4%) and NPV (14.3%) were observed among this subgroup, so that also in cytologically suspicious for malignancy nodules RAS testing could not represent a reliable rule-out test. In cytologically indeterminate subgroup, where MR was 34%, SE and PPV of RAS testing were low (below 60% and 45%, respectively), affecting its accuracy as a rule-in and rule-out test. Similarly, low values of both SE and PPV were recently reported by Wu et al. [23], who explored the diagnostic value of KRAS mutation in cytologically indeterminate nodules. We therefore confirmed that RAS mutations were not specific for malignancy.
As concerns TIRADSs, at the high risk (category 5) ultrasound category threshold, we found overlapping diagnostic value of four TIRADSs (ACR, EU, K and ATA US-based RSS) alone and in combination with RAS testing, and irrespective of cytology. TIRADSs alone showed moderate accuracy (69.0% in cytologically indeterminate and 45.8% in suspicious for malignancy thyroid nodules) since they were unsatisfactory as “rule-out test”. In other words, although we found a relatively high SPEC and PPV for the preoperative ultrasonographic identification of nodules with suspicious features, most of the histologically follicular cancers evaluated in this series were missed by ultrasound. Our findings showed that while suspicious ultrasonographic features are useful when present, most RAS-positive cancers lack suspicious features of any type. These findings were in line with those of Wang et al. [30].
Moreover, when we explored the value of the four TIRADSs in combination with RAS testing we obtained a non-significant improvement of accuracy in cytologically suspicious for malignancy thyroid nodules and a non-significant worsening of accuracy in cytologically indeterminate nodules (Table 5). Specifically, in cytologically indeterminate nodule, although being an absolute amelioration of SE, we found a relevant decrease in SPEC and PPV.
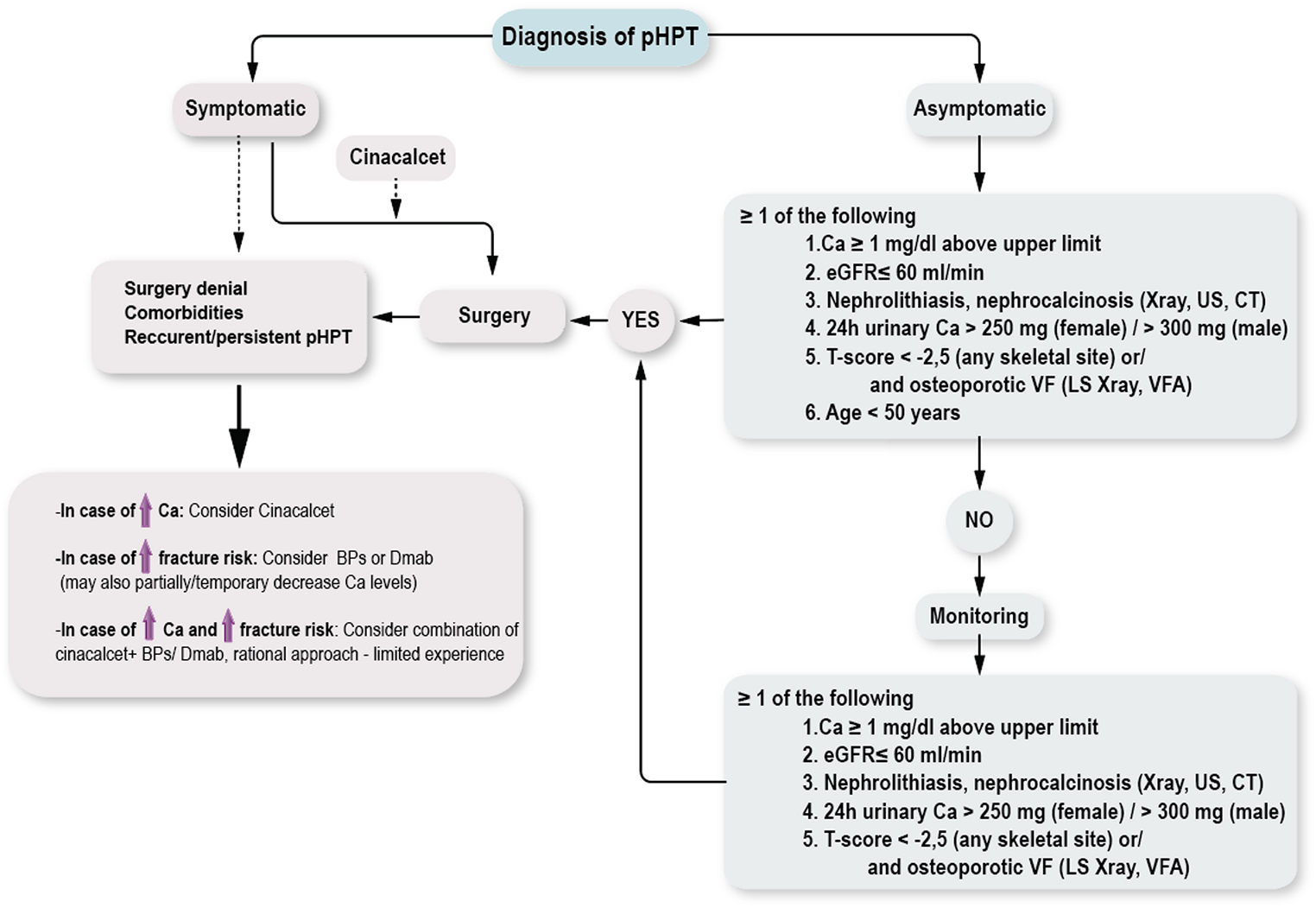
As illustrated in Fig. 3, our final aim was to show how TIRADSs and RAS testing could integrate in a clinical scenario. Specifically, in cytologically suspicious for malignancy thyroid nodules, when dealing with sonographically high suspicion nodules RAS mutation could not improve malignancy rates. This was due to the high specificity for malignancy of TIRADSs in this context and the possibility to have WILD type testing result being malignant on histology (three cases in our study). Conversely, when facing sonographically non-high suspicion nodules RAS testing improperly would avoid surgery in 9 out of eleven WILD type nodules, while correctly would indicate surgery in 4 out of 4 RAS + cases. Therefore, this altogether meant that, in cytologically suspicious for malignancy thyroid nodules, RAS testing would have correctly diagnosed malignancy in only one case more than the four TIRADSs. In cytologically indeterminate thyroid nodules, when facing sonographically high suspicion nodules RAS testing correctly diagnosed four malignancies while improperly would avoid surgery in three cases. Furthermore, when facing sonographically non-high suspicion nodules if on one side RAS testing correctly indicated surgery in 16 cases and correctly avoided surgery in 36 cases, on the other side it improperly indicated surgery in 28 cases and improperly avoided surgery in 13 cases. Therefore, this altogether meant that, in cytologically indeterminate thyroid nodules, RAS testing would have correctly diagnosed malignancy in 15 cases more than the four TIRADSs but would have improperly indicated surgery in 26 cases more than the four TIRADSs. All this meant that RAS mutations and US-based RSSs, taken singly, are limited at differentiating malignant from benign indeterminate nodules, as well as their combination. The major limitation of both suspicious sonographic features and/or mutational markers was their relatively low occurrence in malignant indeterminate nodules [22].
There are limitations of our study that warrant some caution. First, there was an unavoidable selection bias because the data were retrospectively evaluated, and surgery and molecular testing were not always available. Second, the study has a single-center experience that cannot account for geographic variations in incidences of thyroid cancer or thyroid cancer subtypes. Third, our findings only referred to isolated RAS mutations, failing to explore the diagnostic value of RAS mutations with other molecular alterations [19, 21]. Fourth, this series was limited to nodules with operative treatment, which may have contributed to referral bias. Fifth, our results derived from the ultrasound data could be different in other centers also because of the moderate interobserver variability [34]. However, the use of US-based RSSs is deemed to significantly improve interobserver agreement in assessing thyroid nodules [35]. Sixth, this study relied on static image analysis, which could introduce a certain degree of bias during the classification process.
Our study’s strengths are multiple. First, all the histologic outcomes were after the advent of NIFTP [36], properly reporting the final diagnosis and avoiding false diagnoses of follicular variant of PTC [33]. Second, our findings were representative of the four main US-based RSSs for the first time, alone and in combination with RAS mutations, since we tested two pattern-based TIRADSs (ETA and ATA) and two score-based TIRADSs (ACR and KOREAN), and we found overlapping results among these four RSSs. Third, our protocol was designed to also explore diagnostic value of cytologically suspicious for malignancy nodules, since future investigations into clinical utility of RAS mutations across other cytological categories are warranted to strengthen the evidence of ATA guideline recommendations 17a and 20 [1, 19]. Fourth, our anatomic pathologists were formally blinded to histologic or molecular results, which could not introduce bias; similarly, the revision of US images was performed blinded to the other results.





Comments (0)