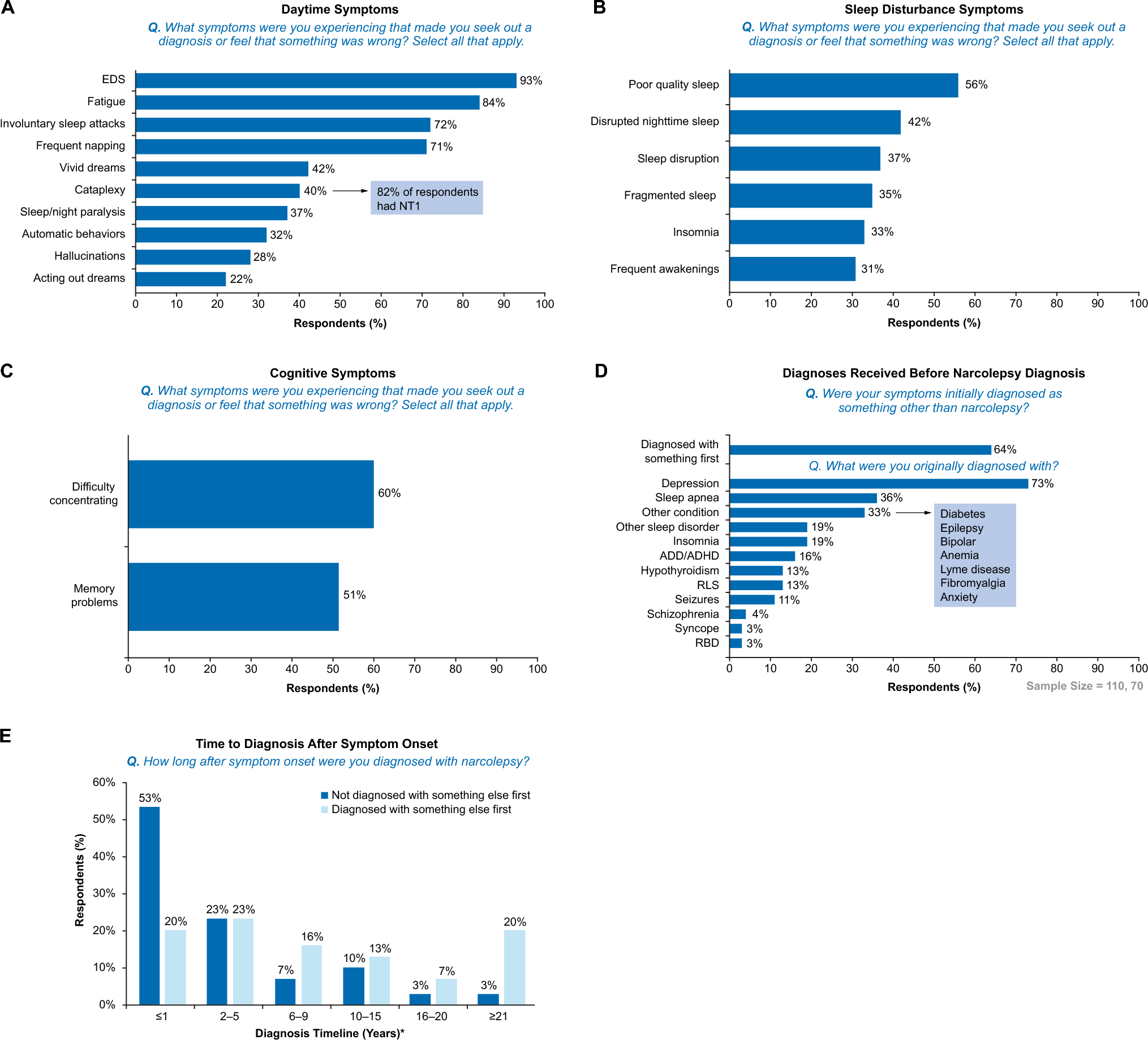
On their journey to a narcolepsy diagnosis, PWN routinely experienced a misdiagnosis or a “missed” diagnosis. One-third of respondents received disparate initial diagnoses that included anxiety, bipolar disease, epilepsy, fibromyalgia, anemia, and Lyme disease. As many of these conditions (e.g., sleep apnea and epilepsy) require objective diagnostic testing, these survey findings underscore the potential for complex comorbidities in PWN that lead to “missed” diagnoses of narcolepsy [10, 11]. Initial diagnoses based on subjective criteria and symptom presentation, such as insomnia, may contribute to an array of possible misdiagnoses by clinicians [10]. Clinicians often do not have expertise in narcolepsy, owing to limited disease awareness and lack of sleep training in general medical education [12, 13]. Given these experiences, it is not surprising that participants sought out information from a variety of resources, such as websites and advocacy groups. For example, nearly 50% of participants used scientific articles as a resource. This introduces an opportunity for patients and clinicians to share awareness of available resources and reinforces the need to make resources accessible, ideally as peer-reviewed plain language summaries, to empower people living with narcolepsy to guide their own care.
More than half of respondents experienced symptoms of narcolepsy within the first two decades of life, underscoring that narcolepsy is often a pediatric disease [14], and education of pediatricians, school faculty, and parents is essential to shorten the time to referral and adequate evaluation and diagnosis by sleep clinicians. In this study, approximately 40% of respondents received a diagnosis between 2 to 9 years from the initial consultation with a clinician regarding their symptoms, and nearly one-third waited ≥ 10 years. These findings align with a recent registry study that estimated an average time of 4.5 years from first consultation to diagnosis using self-reported data in adult PWN [10]. Prior to diagnosis, the majority of PWN, irrespective of narcolepsy type, were suffering from a sleep disturbance, characterized by either poor quality sleep, DNS, sleep disruption, fragmented sleep, insomnia, or frequent awakenings, highlighting the 24-h nature of narcolepsy. These symptoms, particularly when described in a primary care setting, may distract from considering narcolepsy. Most respondents with a definitive NT1 diagnosis experienced consistent episodes of cataplexy that were often triggered by feelings of being overtired, which is consistent with existing literature reporting an association between “tiredness” and more frequent cataplexy [15]. Overtiredness, which may be more common in PWN, may increase an individual’s susceptibility to a cataplexy episode based on an emotional trigger. While clinicians educate PWN about emotions and cataplexy, greater awareness around overtiredness predisposing a person to cataplexy episodes may be needed. Further, a consistent sleep routine, with naps as needed, should be encouraged as a behavioral strategy for PWN.
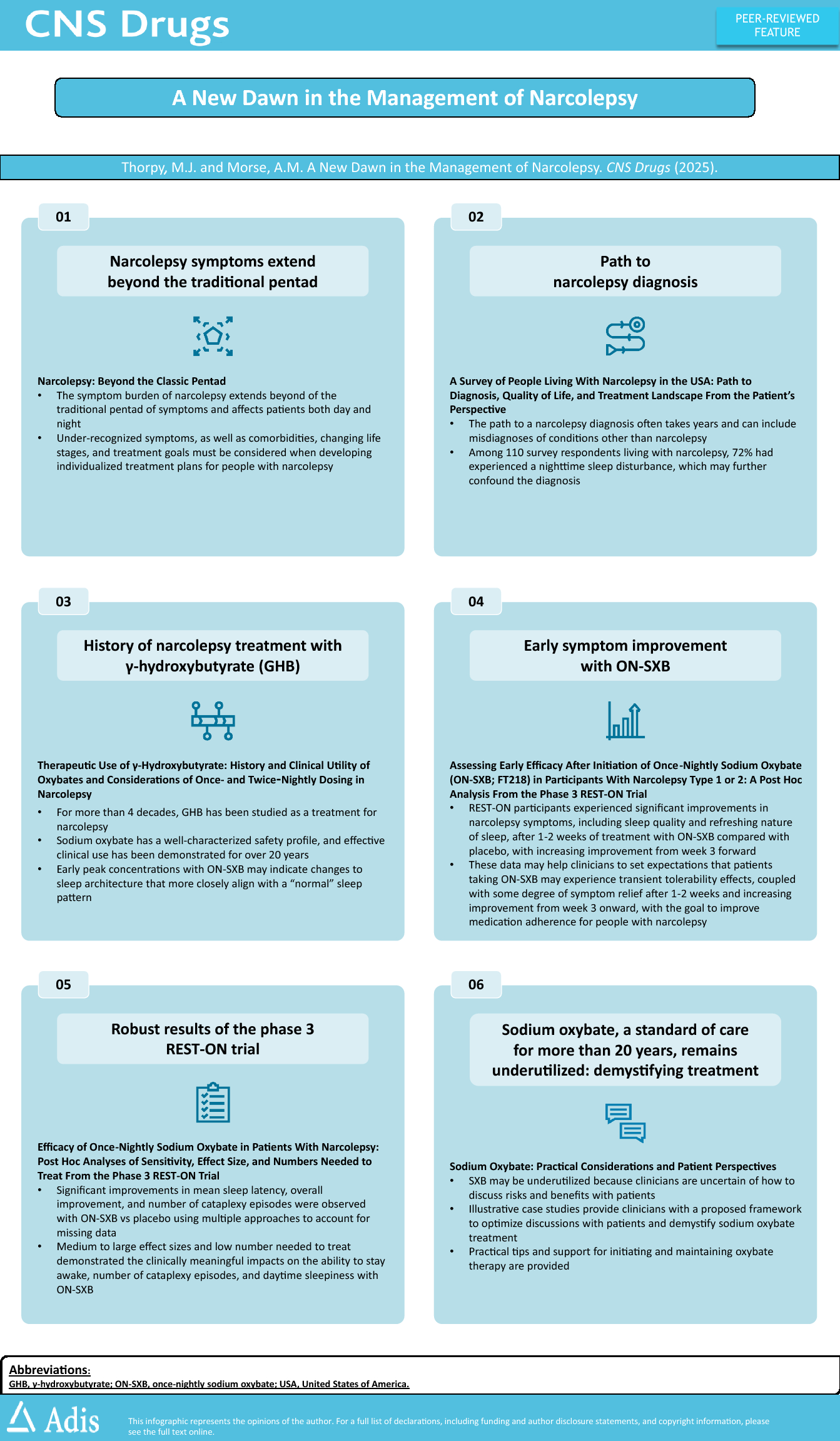
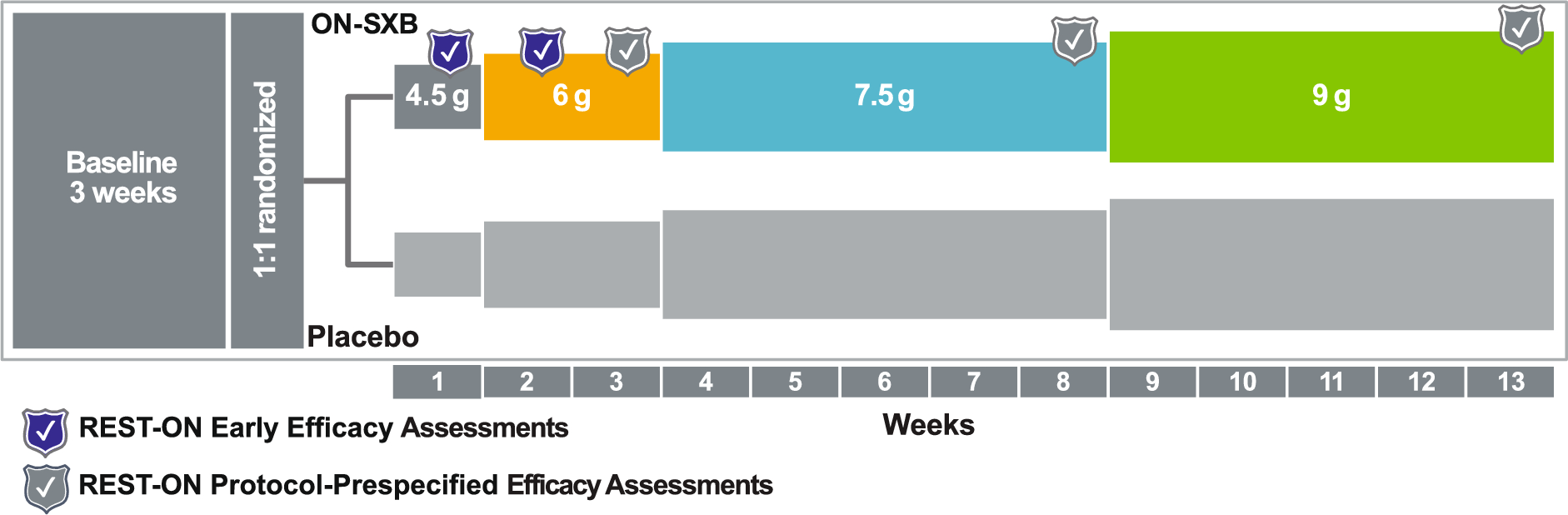
Overall, many respondents indicated that narcolepsy imposed a significant negative impact on their personal and professional lives, especially when contending with the emotional toll associated with narcolepsy. Polypharmacy was common and likely reflective of the invasive, 24-h nature of narcolepsy and desire of PWN to experience relief from a wide range of both daytime and nighttime symptoms. Sleeping through the night was a desired treatment goal among all survey respondents, but particularly among those who were taking an immediate-release oxybate medication. Given the twice-nightly dosing regimen of immediate-release oxybates [16, 17], these formulations may hinder the ability of patients to achieve their desired treatment goals. Notably, a once-nightly, extended-release formulation of sodium oxybate has been approved by the US Food and Drug Administration (FDA) for the treatment of narcolepsy in adults and children, eliminating the need for a second, middle-of-the-night dose [18]. Importantly, this survey reveals that many PWN in the USA are self-motivated and seek out additional information and resources to augment their understanding of narcolepsy, as well as options available for symptom improvement. Owing to the complexities in the diagnosis of narcolepsy, treatments, and the associated comorbidities, PWN often utilized ongoing resources and education. Supplementary internet sources were most commonly utilized.
Real-world evidence obtained through the lived experience of PWN clearly illustrates that narcolepsy is a challenging disorder related to its multiple and varying symptoms, and optimal management of these symptoms can be difficult. Low treatment adherence is common among PWN [19]. Adherence directly impacts the ability of PWN to achieve optimal outcomes, and with most respondents requiring polypharmacy, there is greater treatment burden, increased risk of adverse events, and risk of drug–drug interactions [20]. While polypharmacy often results from inadequate response to narcolepsy treatment [21], failure to recognize nonadherence may also contribute to use of multiple medications in some PWN. In the present study, most respondents reported experiencing a multitude of troubling pentad and non-pentad symptoms including EDS, fatigue, difficulty concentrating, and memory impairment. Notably, more than half of the respondents considered one or more sleep disturbances as their most troubling symptoms, with poor sleep quality, DNS, and frequent awakenings among the top ten; daytime medications, especially traditional stimulants, may contribute to these underlying sleep disturbances [22].
Approaches to address sleep-related issues varied. Melatonin, an over-the-counter sleep supplement, was the most commonly used sleep-related treatment, reported by approximately 16% of respondents. Almost 20% of respondents receiving an amphetamine-based alerting agent reported melatonin use. Limited information is available about endogenous or exogenous melatonin for PWN. Endogenous melatonin and circadian rhythm may be dysregulated in some PWN [23]. In general, exogenous melatonin has been used to alter ultradian rhythm in PWN and people without narcolepsy; however, exogenous melatonin can increase time spent in REM sleep [24]. While there are reports suggesting that melatonin may be of use in treating RBD in PWN [25, 26], there is no clinical evidence of its efficacy in narcolepsy. Additionally, the content of melatonin in supplements is frequently inconsistent with that indicated on the label [27].
PWN were frequently treated with stimulants such as dextroamphetamine or dextroamphetamine–amphetamine, whereas interventions strongly recommended by the American Academy of Sleep Medicine (e.g., modafinil, pitolisant, sodium oxybate, and solriamfetol) [28] were underutilized (3–20% of respondents). Together, these findings suggest that opportunities exist for improvement in the care of PWN and highlight the persistent use of stimulants, which have historically been used to treat EDS [29], despite their addiction potential and potential to increase blood pressure and heart rate. Education of and advocacy to managed care organizations about the need for access to additional medications that are aligned with the American Academy of Sleep Medicine guidelines continue to be needed.
The presence of cataplexy is a defining feature of NT1 that results from an underlying dysregulation of sleep–wake states and intrusion of REM sleep-related atonia during wakefulness, which manifests with muscle atonia [30]. Ensuring clinicians use understandable and wide-ranging descriptions to explain cataplexy is critical; suggested language for clinical use can be found in the companion article by Lavender et al. [31]. In the present study, 6% of respondents with NT2 reported that they had experienced cataplexy compared with 68% of respondents with NT1. This potentially highlights a discrepancy between the specificity of cataplexy in the pathophysiology of NT1 and the perception of a cataplexy episode by the patient themselves. As reported previously, this may be due to the large phenotypic diversity of cataplexy among PWN and the corresponding difficulty to adequately recognize and diagnose cataplexy in clinical practice [15, 32]. Further, cataplexy may be confused with other disorders such as epileptic seizures, falls from neuromuscular disorders [33], and syncope [34], suggesting that there remains an unmet need to provide PWN definitive criteria to determine the presence of a cataplexy episode. Given that 27% of respondents who were not sure of their narcolepsy type reported cataplexy as their most troubling symptom, respondents with NT1 may be underdiagnosed. In this study, respondents with NT1 were commonly prescribed venlafaxine (15%) and fluoxetine (13%). Antidepressants are commonly used off-label to manage cataplexy symptoms in PWN; however, limited evidence is available to support a favorable risk–benefit profile, and the American Academy of Sleep Medicine does not include antidepressants in its guidelines, on the basis of limited data [5, 28, 35]. While the American Academy of Sleep Medicine guidelines do not recognize antidepressants, the European Narcolepsy Guidelines recognize both sodium oxybate as monotherapy and antidepressants as strong recommendations for cataplexy treatment [36].
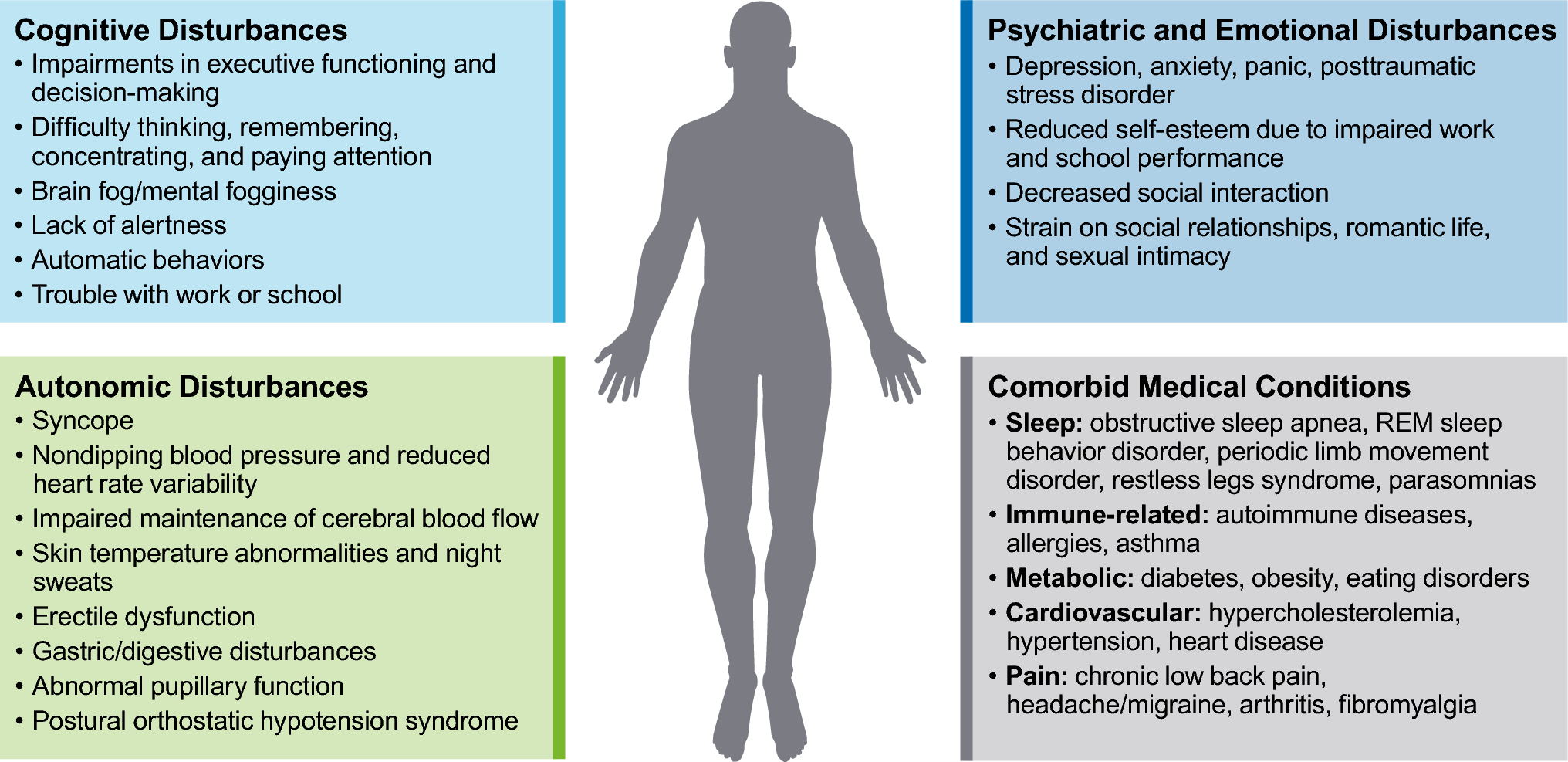
PWN experienced a broad impact on their QoL, reporting interference across several domains including work, social life, daily activities, emotional well-being, cognition, and exercise. In this study, the majority of respondents reported an extremely or very severe impact. In agreement with these findings, a recent review has indicated that the disease burden of narcolepsy is significantly and negatively correlated with key factors associated with health-related QoL (HRQoL) including physical functioning, general health, and social functioning [37]. Of note was the emotional toll experienced by respondents, with feelings of isolation, depression, and anxiety; many desired the development of treatments that address the underlying etiology of narcolepsy given its debilitating symptom burden. Recommending that PWN consider additional emotional support from peer advocacy groups is needed to help reduce feelings of isolation.
There are several strengths and limitations of this study. The approach gathered voluntary responses from individuals currently living with narcolepsy in an online social network dedicated to people living with narcolepsy, where PWN may be more candid than in a healthcare encounter, providing valuable insight into real-world perceptions of disease burden and treatment. The survey used mostly multiple-choice questions, which likely encouraged potential respondents to participate but may have restricted patient responses. Additionally, this study utilized a nonvalidated questionnaire, which may limit the reliability and consistency of the results; patient-reported data may be susceptible to misinformation or bias. These data represent a sample of US-based individuals aged ≥ 21 years with relative lack of detailed socioeconomic and demographic information; further, the respondents were overwhelmingly female (> 80%). Thus, generalizability to PWN who have differing characteristics or who reside in other countries may be limited. An additional limitation is the self-reporting of narcolepsy type by respondents, as many reported symptoms discordant with their diagnosis or were not sure of their diagnosis at all. Notably, some members of MyNarcolepsyTeam have reported being underdiagnosed only to learn through organic conversations that they are actually experiencing cataplexy, further suggesting that some survey respondents may have been incorrectly diagnosed with NT2. In the present study, several respondents who had cataplexy prior to diagnosis did not indicate cataplexy as a troubling current symptom, and a small number of respondents who did not have cataplexy prior to diagnosis reported that it was now a concern; these findings provide further evidence that narcolepsy symptoms and patient perception of these symptoms may change over time [38]. Owing to the low response rate in this study, these findings may not reflect the broader population of PWN in the USA.


Comments (0)