2.1 Study Design and Participants
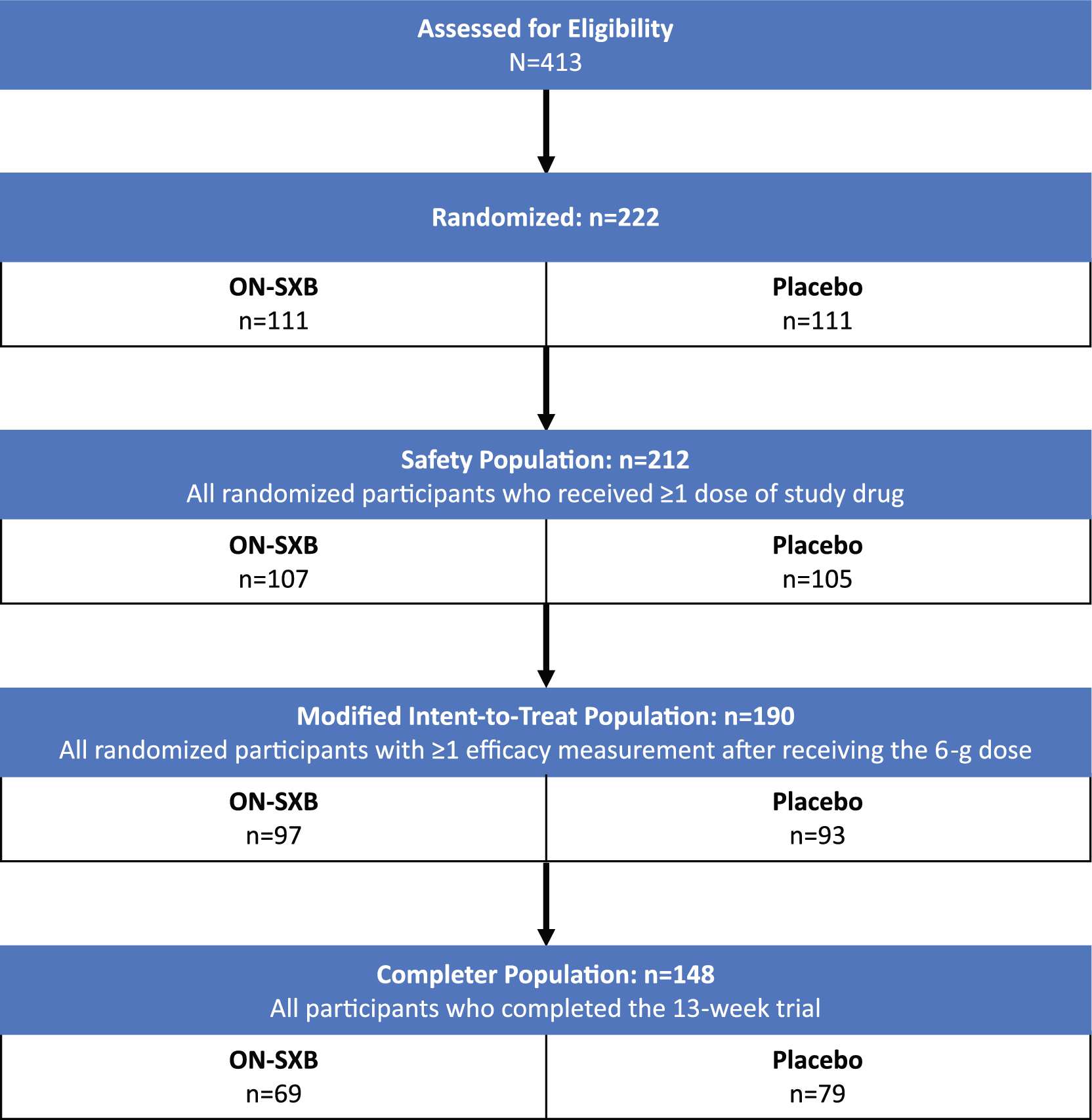
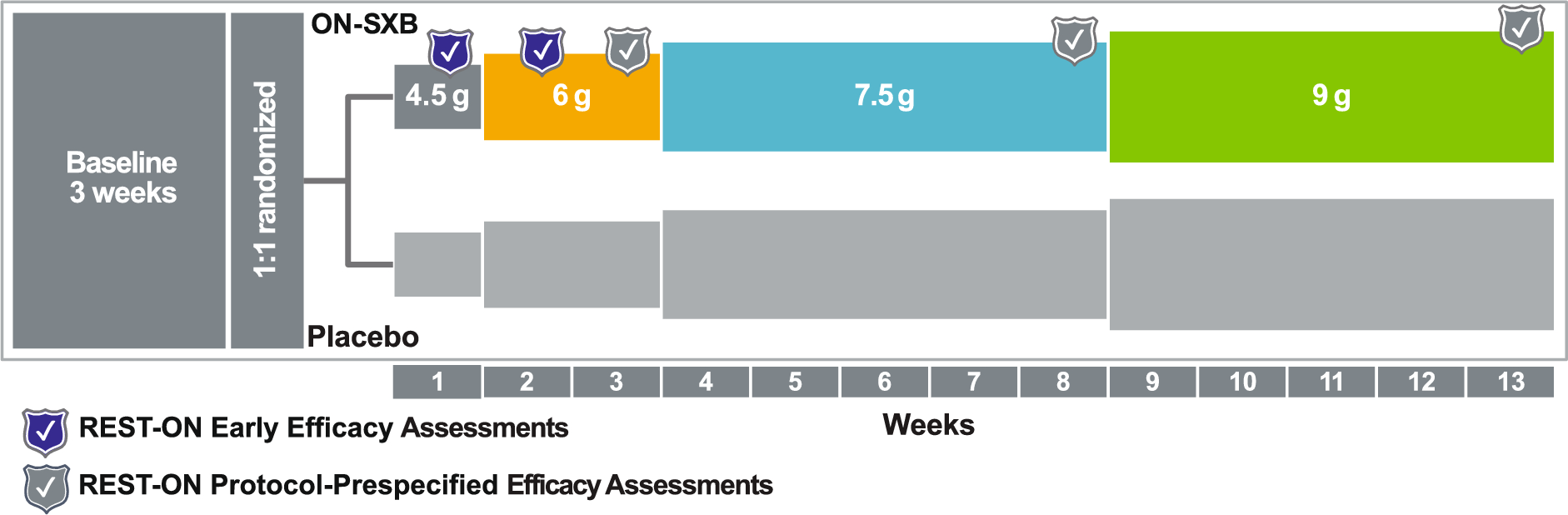
The full details of REST-ON (NCT02720744), a double-blind, placebo-controlled, multicenter clinical trial evaluating the efficacy and safety of ON-SXB for the treatment of narcolepsy, have been reported previously [7]. Briefly, participants aged ≥ 16 years and stratified by narcolepsy type were randomly assigned to receive ON-SXB or placebo in a 1:1 ratio. After a 3-week screening period, participants received treatment with ON-SXB or placebo over 13 weeks (4.5 g for week 1, 6 g during weeks 2–3, 7.5 g during weeks 4–8, and 9 g during weeks 9–13) and were followed for 1 additional week. The study design allowed for the assessment of efficacy and safety of each dose level within the same participant [7].
Eligible participants had a diagnosis of either narcolepsy type (NT) 1 (narcolepsy with cataplexy) or NT2 (narcolepsy without cataplexy), according to the International Classification of Sleep Disorders (Third edition) [7, 16]. Key inclusion criteria were the continued presence of EDS for the preceding 3 months and an ESS score > 10, as well as the continuing presence of cataplexy (participants with NT1 only) for the previous 3 months. Participants using concomitant alerting agents must have had stable dosing for ≥ 3 weeks prior to screening, and the medication regimen was required to remain the same for the duration of the trial. Individuals were initially excluded from REST-ON if they had previously used SXB. The protocol was later amended to allow prior use of SXB ≤ 4.5 g per night for < 2 weeks and ≥ 1 year before entering the study [7].
The REST-ON trial was approved by the institutional review board or ethics committee at each study center and conducted in accordance with the ethical principles of the Declaration of Helsinki, Good Clinical Practice guidelines, International Council for Harmonisation guidelines, and applicable regulatory requirements at the national and local level. Written informed consent was obtained from all adult participants (≥ 18 years old); participants aged 16 or 17 years provided assent with written informed consent provided by their legal representative [7].
2.2 Assessments
In REST-ON, efficacy endpoints were assessed at baseline and at weeks 3 (6 g dose), 8 (7.5 g dose), and 13 (9 g dose) [7]. Mean sleep latency on the MWT was assessed as the average of five 30-min trials, with each trial terminating immediately after sleep onset or at 30 min in the case of no sleep. The CGI-I assessed the proportion of participants whose overall condition was rated by the clinician as “much improved” or “very much improved” from baseline, measured on a 7-point Likert scale, with a score of 1 indicating “very much improved” and a score of 7 indicating “very much worse.” The mean weekly number of cataplexy episodes was determined for participants with NT1 using the cataplexy item from the Sleep and Symptom Daily Diary. Subjective evaluation of EDS was performed using the ESS, in which participants rated their likelihood of dozing off during eight daily activities on a 4-point scale ranging from 0 (never) to 3 (high), with a higher total score indicating greater sleepiness.
2.3 Statistical Analysis
Methods for the primary analysis of the REST-ON trial have been reported previously [7]. In brief, all primary efficacy analyses were conducted in the mITT population (n = 190), which included all randomized participants who had ≥ 1 efficacy measurement after receiving the 6 g dose of ON-SXB or placebo. MWT, cataplexy, and ESS data were analyzed with a mixed-effects model for repeated measures (MMRM). A logistic regression model for binomial data with logit link was used to analyze CGI-I data.
The post hoc sensitivity analyses for handling missing data reported here include evaluation of the coprimary endpoints of mean sleep latency on the MWT, the proportion of participants who were “much” or “very much” improved on the CGI-I, and the mean weekly number of cataplexy episodes. These endpoints were evaluated in an analysis of all participants who completed the 13-week REST-ON trial (completer population) and in the mITT population via the following analyses: placebo-based multiple imputation (MI) with a missing-not-at-random assumption, analysis of covariance (ANCOVA), and tipping-point–based MI of worsening values. Analyses of the MWT and number of cataplexy episodes evaluated changes from baseline at weeks 3 (6 g), 8 (7.5 g), and 13 (9 g); CGI-I analysis evaluated the proportion of participants with CGI-I ratings of “much” or “very much” improved at the same three time points and dose levels. All analyses that assessed the endpoint regarding number of cataplexy episodes included only those participants with NT1.
For the completer analysis, least squares mean differences (LSMDs), 95% confidence intervals (CIs), and P-values were calculated for change from baseline in mean sleep latency on the MWT and mean weekly number of cataplexy episodes. Odds ratios (OR), 95% CIs, and P-values for the proportion of participants who were “much” or “very much” improved on the CGI-I were also calculated.
In the placebo-based MI analysis, missing values in both treatment groups were imputed from values observed in the placebo group by assuming values were missing not at random. All ANCOVA models included the response variable associated with the endpoint, the fixed effects of treatment visit, treatment by visit, site (US or non-US), and the covariate of the baseline value for the response variable. The tipping-point MI analysis was performed to identify the outcome value at which the statistical significance of the model would be overturned (i.e., P > 0.05). For the placebo-based MI analysis, LSMDs for ON-SXB versus placebo, 95% CIs, and P-values were calculated for the MWT and cataplexy endpoints; ORs, 95% CIs, and P-values were calculated for the CGI-I endpoint. For the ANCOVA, LSMDs for ON-SXB versus placebo, 95% CIs, and P-values were calculated for all three coprimary endpoints. P-values were generated using Rubin’s formula with 100 imputations for the three coprimary endpoints evaluated with the tipping-point–based MI analysis. Statistical significance was assessed using a two-sided α test at a 5% significance level.
Effect size analysis [17] was performed by calculating Cohen’s d from the LSMDs for response of ON-SXB versus placebo in the mITT population on the endpoints of mean sleep latency on the MWT, mean weekly number of cataplexy episodes, and ESS score. All ON-SXB doses (6, 7.5, and 9 g) were assessed and compared with placebo. NNTs were calculated for response of ON-SXB versus placebo in the mITT population on the three coprimary endpoints of REST-ON, identifying the number of participants who need to be treated to obtain one additional responder.
For this post hoc analysis, participants were considered responders if their mean sleep latency increased from baseline by ≥ 5 min on the MWT, their ESS score was ≤ 10, or their mean weekly number of cataplexy episodes declined from baseline by ≥ 50% (participants with NT1). Thresholds were chosen before running the analysis.


Comments (0)