
Remember me

The sleep disorder was first described in the medical literature by Dr. Karl Friedrich Otto Westphal in 1877, with French physician and neurologist Jean-Baptiste-Édouard Gélineau using the term “narcolepsy” in 1880 [1]. The word “narcolepsy” comes from the Greek words “narcosis” (meaning drowsiness) and “lepsis” (meaning attack), which is derived from “lambanein” (meaning to seize or to take) [1, 2].
As with other areas of medicine, tremendous advances have been made in understanding the diagnosis and treatment of narcolepsy from the initial description nearly 150 years ago. Arguably, the last 25 years have been a renaissance in the field of narcolepsy research. Critical advances have been made since the early 2000s, with clarification of the spectrum of disease that exists with the diagnosis of narcolepsy, the identification of the most cited etiology of narcolepsy type 1 (NT1), or narcolepsy with cataplexy as a loss of orexin (or hypocretin), a neuropeptide that regulates the sleep–wake cycle [3], and, finally, a growing number of therapeutics becoming available, with ongoing exciting developments in drug discovery and production.
The treatment landscape has progressed from having a limited number of US Food and Drug Administration (FDA)-approved therapeutics to now having multiple classes and formulations, allowing healthcare providers to tailor pharmacotherapy to individual patient needs to manage this debilitating chronic disorder. The prominence of the patient voice and the emphasis on shared decision-making and psychosocial support have become apparent and necessary [4] and should be encouraged to continue. However, there is considerable work that needs to be advanced to optimize patient care and outcomes, particularly in shortening the unacceptably long period of time from symptom onset to accurate diagnosis [4]; clinicians in sleep medicine must continue to educate and advocate for their patients by increasing knowledge and referral to sleep clinicians, improving accessibility and sensitivity of diagnostic paradigms, and continuing to listen to and learn from their patients.
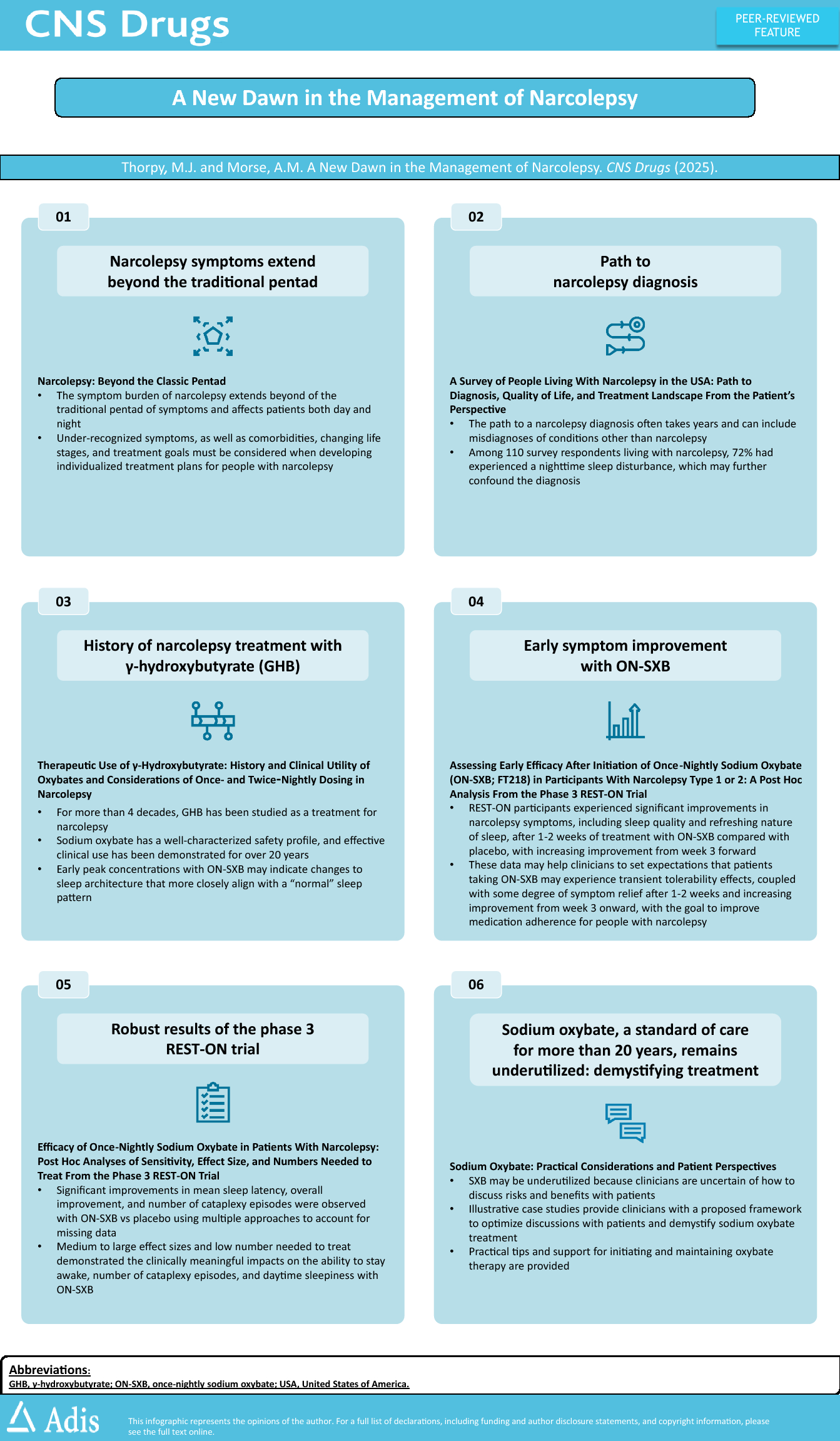
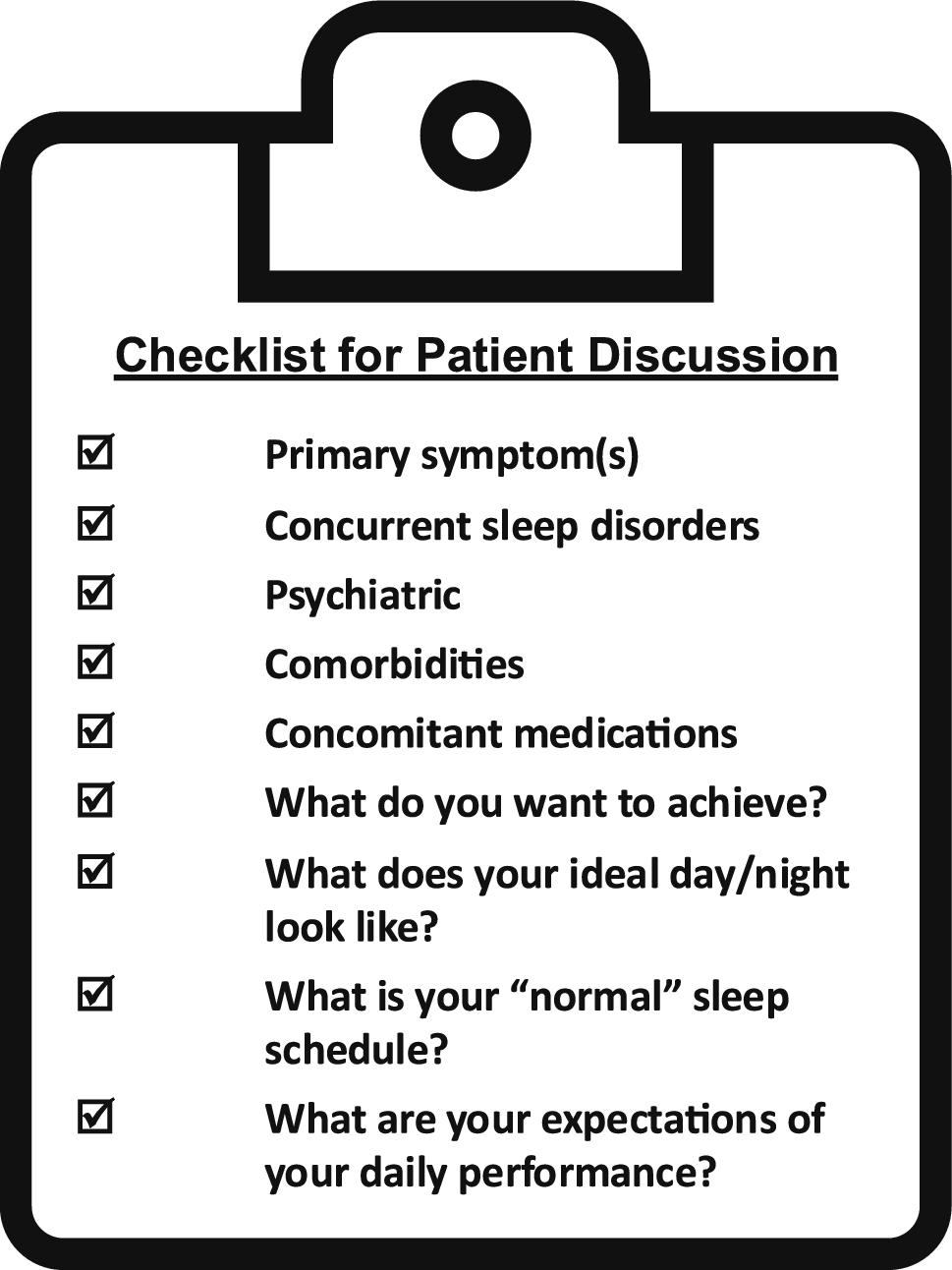
The six publications in this CNS Drugs supplement provide insights on clinical management, shared decision-making, and goal setting for people with narcolepsy and their clinicians (see infographic). A particular emphasis is provided for oxybate therapy, including a historical reference to nearly 50 years ago, when sodium oxybate was first assessed in NT1 and shown to provide remarkable results [5]. Despite sodium oxybate being recognized as a standard of care by the American Academy of Sleep Medicine (AASM)—reaffirmed in 2021 as 1 of 4 medications with a strong recommendation to treat excessive daytime sleepiness (EDS); recognized as 1 of 2 medications with a strong recommendation for both EDS and cataplexy [6]; and additionally having profound efficacy, a well-characterized safety profile, and the availability of multiple formulations [7,8,9]—oxybates remain underutilized.
Education on safety, beyond simply describing adverse reactions, may help to address underutilization. The FDA requires a risk evaluation and mitigation strategy (REMS) for all oxybates to assure safe use owing to the risk of central nervous system depression and respiratory depression, as well as the potential for abuse, misuse, or diversion [10,11,12].
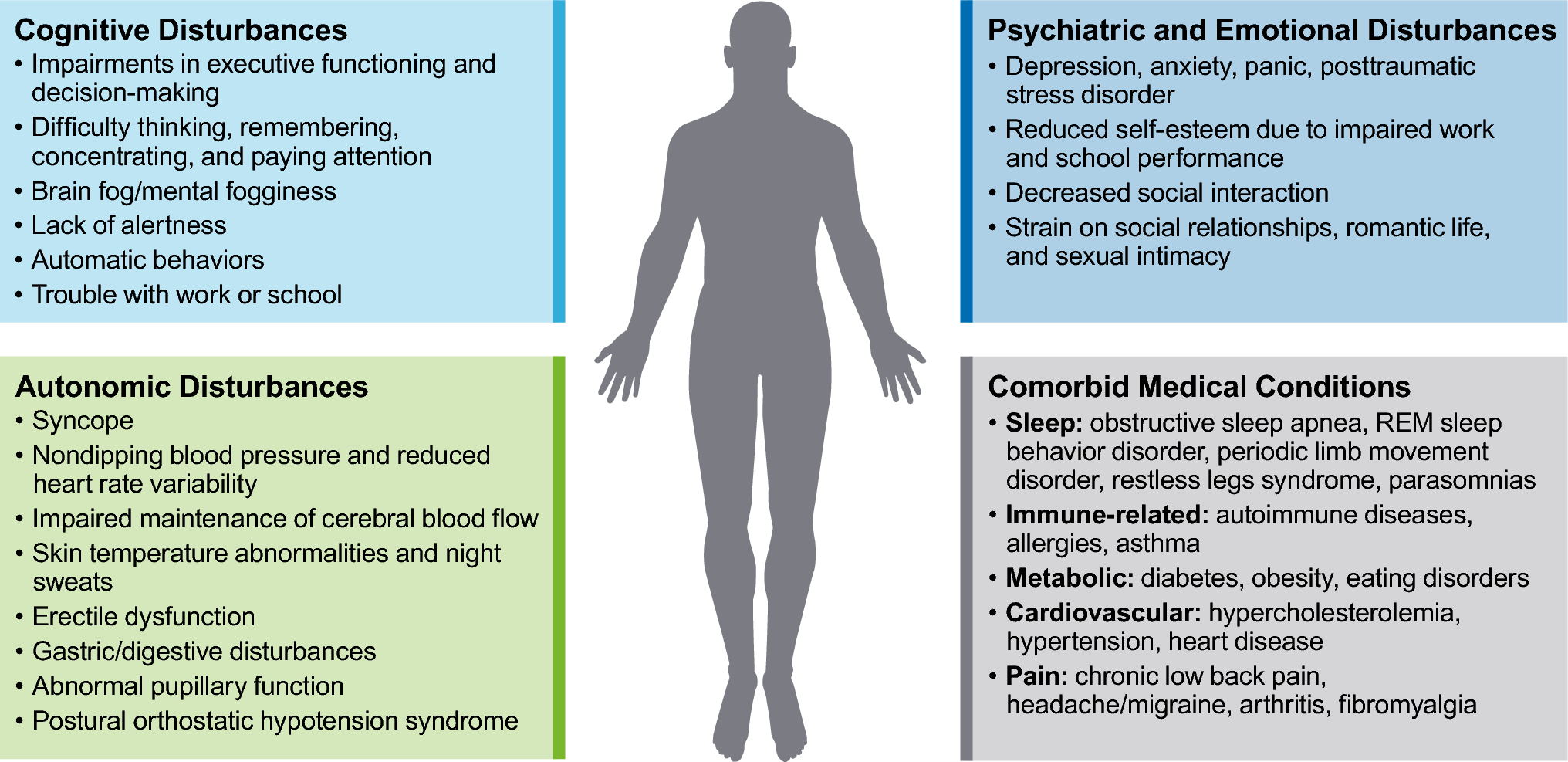
This supplement begins with the five core components of the narcolepsy pentad—EDS, cataplexy, disrupted nighttime sleep, sleep paralysis, and hypnagogic/hypnopompic hallucinations—and then expands to include the additional rapid eye movement sleep-related symptoms, cognitive symptoms, and comorbidities [3], underscoring the need for both the art and science of medicine in this therapeutic area. In the first article, “Narcolepsy: beyond the classic pentad [13],” Dr. Anne Marie Morse and colleagues describe the cognitive, psychiatric, metabolic, and sleep disturbances that may present in narcolepsy, highlighting the need for a comprehensive and patient-specific diagnostic and management approach.
Dr. Thorpy first began practicing sleep medicine in the 1980s and had the privilege of training many fellows, residents, and students, passing on not only his clinical knowledge but also his passion for how sleep clinicians can transform patient lives with appropriate diagnosis and treatment. He has been delighted to see Dr. Morse, as a former sleep medicine fellow, further develop this field of pediatric and adult narcolepsy since she completed her fellowship with him in 2016.
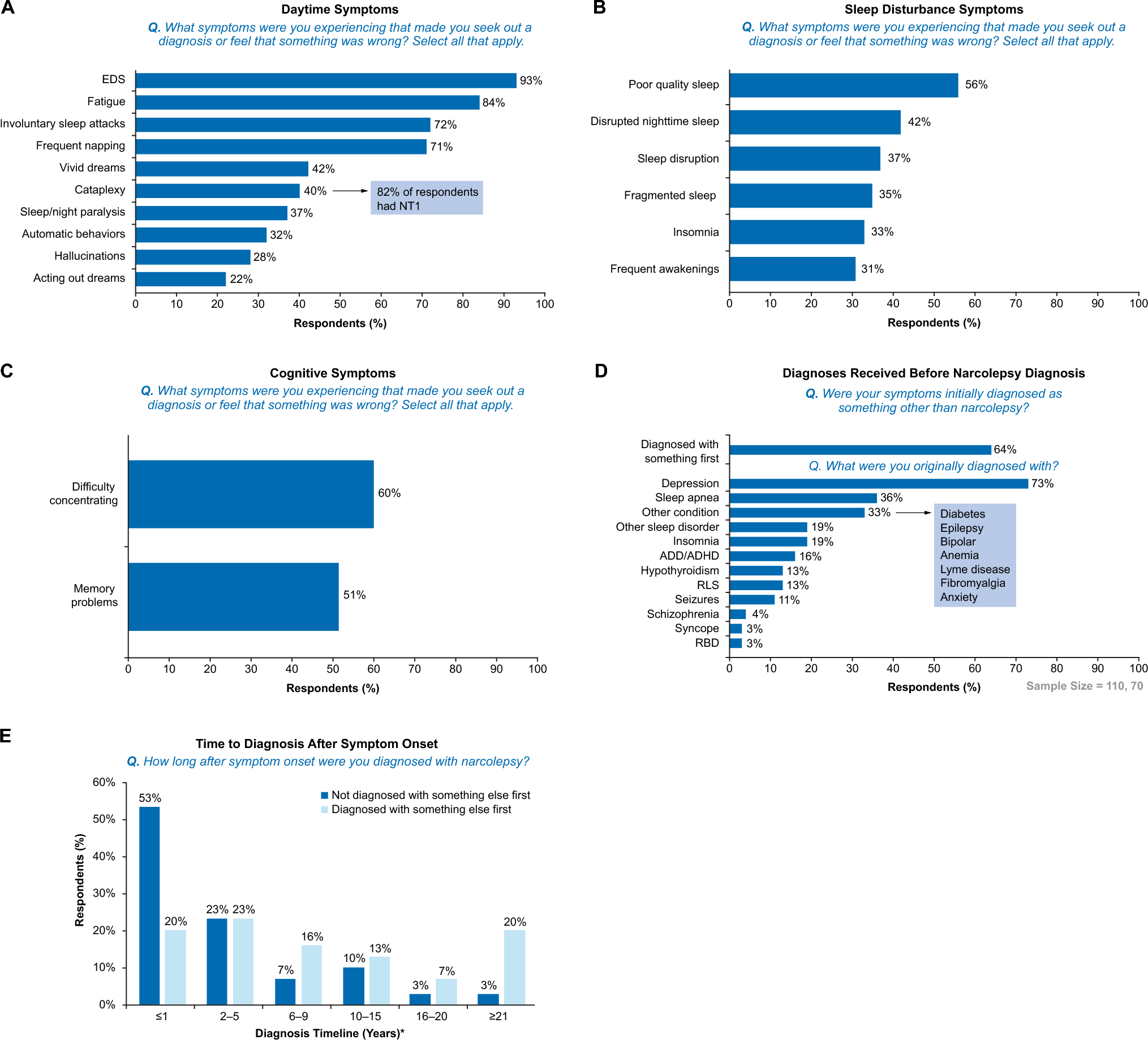
Dr. Morse has been on the vanguard of emphasizing the patient perspective and lived experience through her patient advocacy work and her engagement with thousands on social media. The second publication, “A survey of people living with narcolepsy in the US: path to diagnosis, quality of life, and treatment landscape from the patient’s perspective [14],” authored by Dr. Luis E. Ortiz and colleagues, provides additional insight into the patient journey using new survey data generated from MyNarcolepsyTeam, a closed network of people with narcolepsy, or PWN, as this community may refer to themselves. As lead author, Dr. Ortiz not only provides his input as a pediatric pulmonologist practicing sleep medicine but also shares the unique perspective as a PWN and helps to further contextualize data obtained directly from people living with this chronic disease. Part of the joy—and challenge—of caring for patients with narcolepsy is understanding their similarities (e.g., delayed diagnoses, impact on their employment and personal lives [4], and the need for polypharmacy, including alerting agents [8, 9]) and recognizing the individual patient differences that clinicians must address. Ortiz et al. describe the path to diagnosis and symptom burden experienced by people with narcolepsy, as well as treatment trends and desires, using real-world perspectives. It is expected that many of these will be familiar to clinicians’ in their daily patient care, but some perspectives may further illuminate how clinicians engage with patients.
In the mid-century, methylphenidate and amphetamine-based stimulants were the only options to address EDS [2]. For many patients and providers, these stimulants remain the bedrock of treatment, even in the 2020s [2], despite new classes of medications that are available and recommended by the AASM [6]. While stimulants have been a mainstay of narcolepsy treatment since the mid-1950s [2], identification of sodium oxybate as a potential treatment was pioneered by Broughton and Mamelak, with their 1979 study showing efficacy improving both cataplexy and EDS [5]. It was not until 23 years later, in 2002, that sodium oxybate was FDA-approved for the treatment of cataplexy in narcolepsy and was later expanded in 2005 to include EDS in narcolepsy [10]. This medication, Xyrem® (sodium oxybate, Jazz Pharmaceuticals, Palo Alto, CA), was shown to dramatically improve patient management of narcolepsy symptoms [7]. However, as recognized both by Dr. Mamelak in 1979 [5] and by the FDA Voice of the Patient Drug Development meeting in 2014 [4], sodium oxybate had the drawback of a short duration of action, requiring a unique dosing regimen: administration directly prior to bedtime and a second dose taken 2.5–4 h later [10]. In addition, initial clinician reluctance to use oxybates owing to abuse concerns was gradually overcome over the years by recognition of the excellent efficacy [3] and lack of abuse in patients with narcolepsy [15], underscoring the appropriate way in which the REMS is designed to work. In the third article, “Therapeutic use of γ-hydroxybutyrate: history and clinical utility of oxybates and considerations of once- and twice-nightly dosing in narcolepsy [16],” Dr. Thomas Roth, who has been on the forefront of advancing sleep medicine, describes this background and more, including the long-overdue development of an extended-release form of sodium oxybate (ON-SXB; LUMRYZ™, Avadel Pharmaceuticals, Chesterfield, MO).
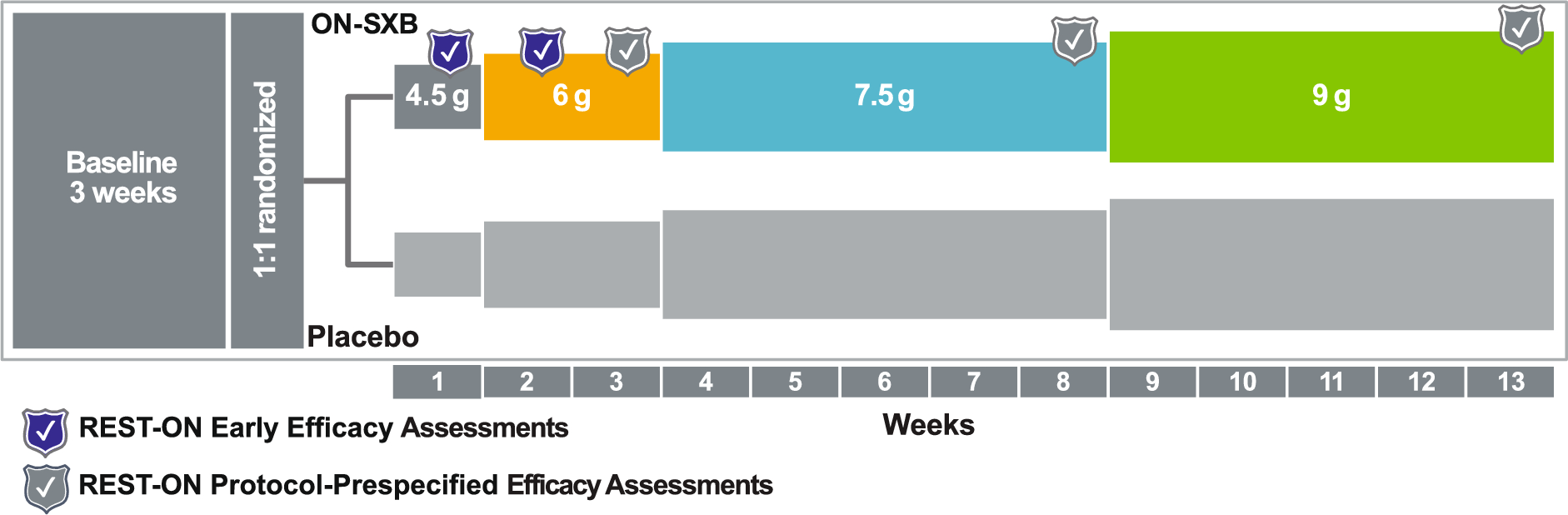
Many sleep clinicians will recognize another giant in the field of sleep medicine, Dr. Lois Krahn. Dr. Krahn and colleagues present post hoc analyses from the pivotal, phase 3, double-blind, placebo-controlled, two-arm, multicenter, randomized REST-ON clinical trial [9], which was the basis of the FDA approval of ON-SXB in 2023 [12], in the fourth paper titled “Assessing early efficacy after initiation of once-nightly sodium oxybate (ON-SXB; FT218) in participants with narcolepsy type 1 or 2: a post hoc analysis from the phase 3 REST-ON trial [17].” During our years in practice, we recognize that setting expectations with patients who are initiating any narcolepsy medication, and oxybates in particular, is critical. All clinicians are encouraged to educate patients on common adverse reactions (e.g., nausea, vomiting, headache, dizziness, and enuresis) [10,11,12] and most importantly, set expectations that these are likely to be transient in nature [9]. Sleep clinicians have a tough job, educating patients and families about oxybates. There is considerable information to relay, and more often than not, considerable misconceptions to debunk, as Dr. Roth describes. One aspect of expectation setting is estimating when benefits are likely to be felt. In this post hoc analysis, ON-SXB treatment effect is shown as early as 2 weeks after initiation, with only the 6-g dose, and maximum effect was observed at the 9-g dose [9].
Despite clinicians’ best counseling efforts, some patients deemed candidates for oxybates may elect—or the clinician may elect—to discontinue oxybate therapy, as occurs in clinical studies of oxybates [7,8,9]. Further research may improve personalized treatment of narcolepsy by identifying patients who are most likely to respond positively to oxybates, as well as those who may experience adverse effects. In the most recent 12-week clinical trials of oxybate, approximately 30% of participants discontinued [8, 9]. In the fifth paper, “Efficacy of once-nightly sodium oxybate in patients with narcolepsy: post hoc analyses of sensitivity, effect size, and numbers needed to treat from the phase 3 REST-ON trial [18],” Dr. Roth and colleagues demonstrate the robustness of the REST-ON efficacy data through multiple post hoc sensitivity analyses that account for missing participant data. On a more practical basis, Roth et al. provide numbers needed to treat, which may be helpful in setting treatment expectations.
This supplement is closed with “Sodium oxybate: practical considerations and patient perspectives [19],” authored by three advanced practice providers, including one who is a person with narcolepsy. Advanced practice providers (i.e., physician assistants or nurse practitioners) have become an integral part of patient care in many therapeutic disciplines [20]. Their training emphasizes partnering with their patients to seek solutions that fit within the patient’s overall health priorities and lifestyle, rather than focusing on a specific diagnosis or chief complaint, and supports patients in ways that complement the role of the physician [20]. Maggie Lavendar, MSN, APRN, FNP-C, et al. provide perspectives in the way clinicians all learn best: with patient cases and practical application of knowledge.
Clinicians who choose to focus on sleep medicine practice in a very special field. Sleep clinicians have the privilege to bear witness to a transformation when partnering with patients. There are many challenging aspects of a sleep clinician’s career (e.g., diagnosis, billing, charting, or insurance calls), but there is a profound effect in successfully treating narcolepsy symptoms and facilitating improvements in people’s lives. Clinicians owe it to their patients to continue their commitment to education on the variability and range of disabling clinical features and manifestations of narcolepsy, to stay apprised of the current developments in the area of pharmacotherapeutics, and to continue to advocate for and with their patients.
FormalPara Infographic:
Comments (0)