
Remember me
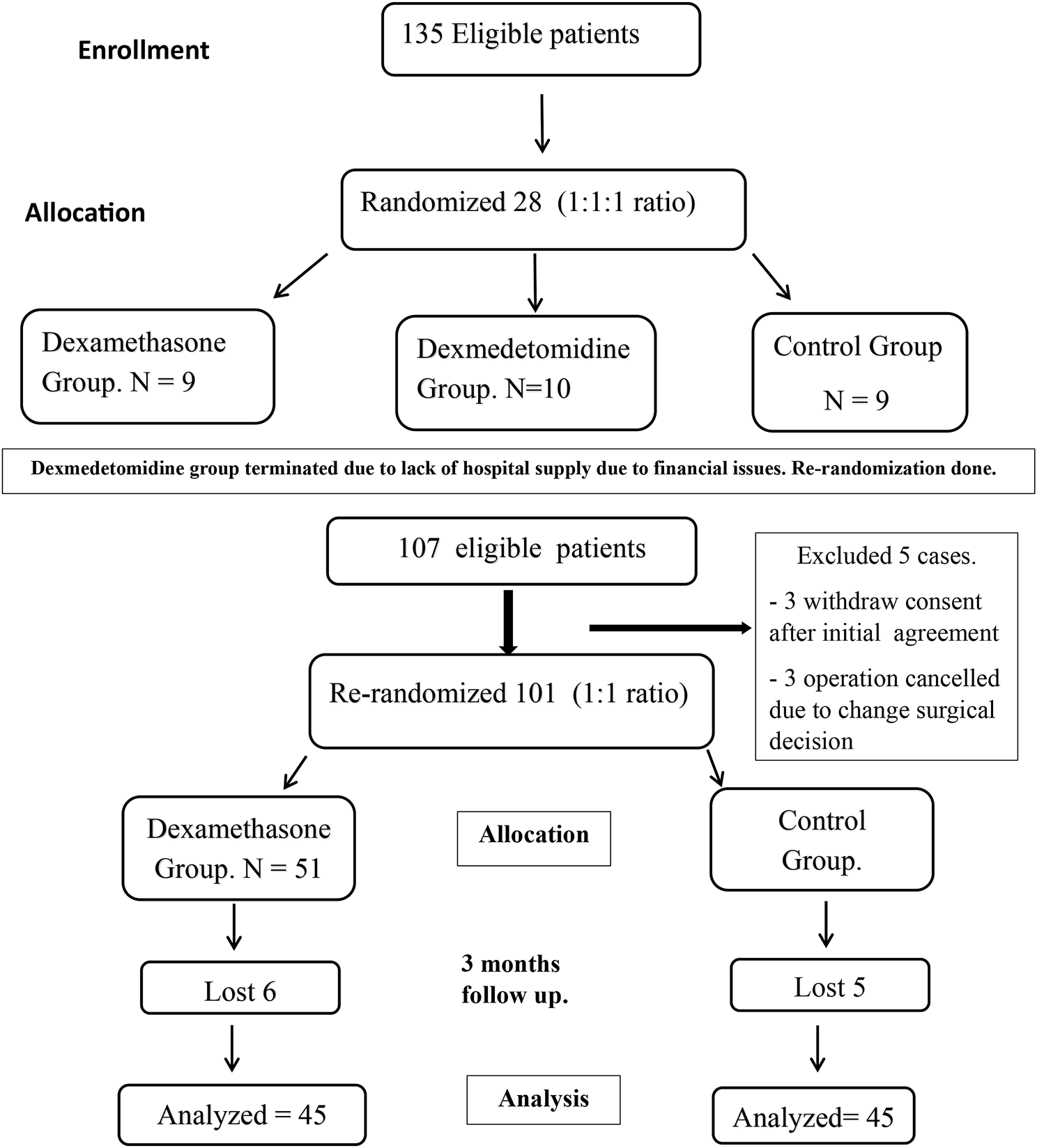


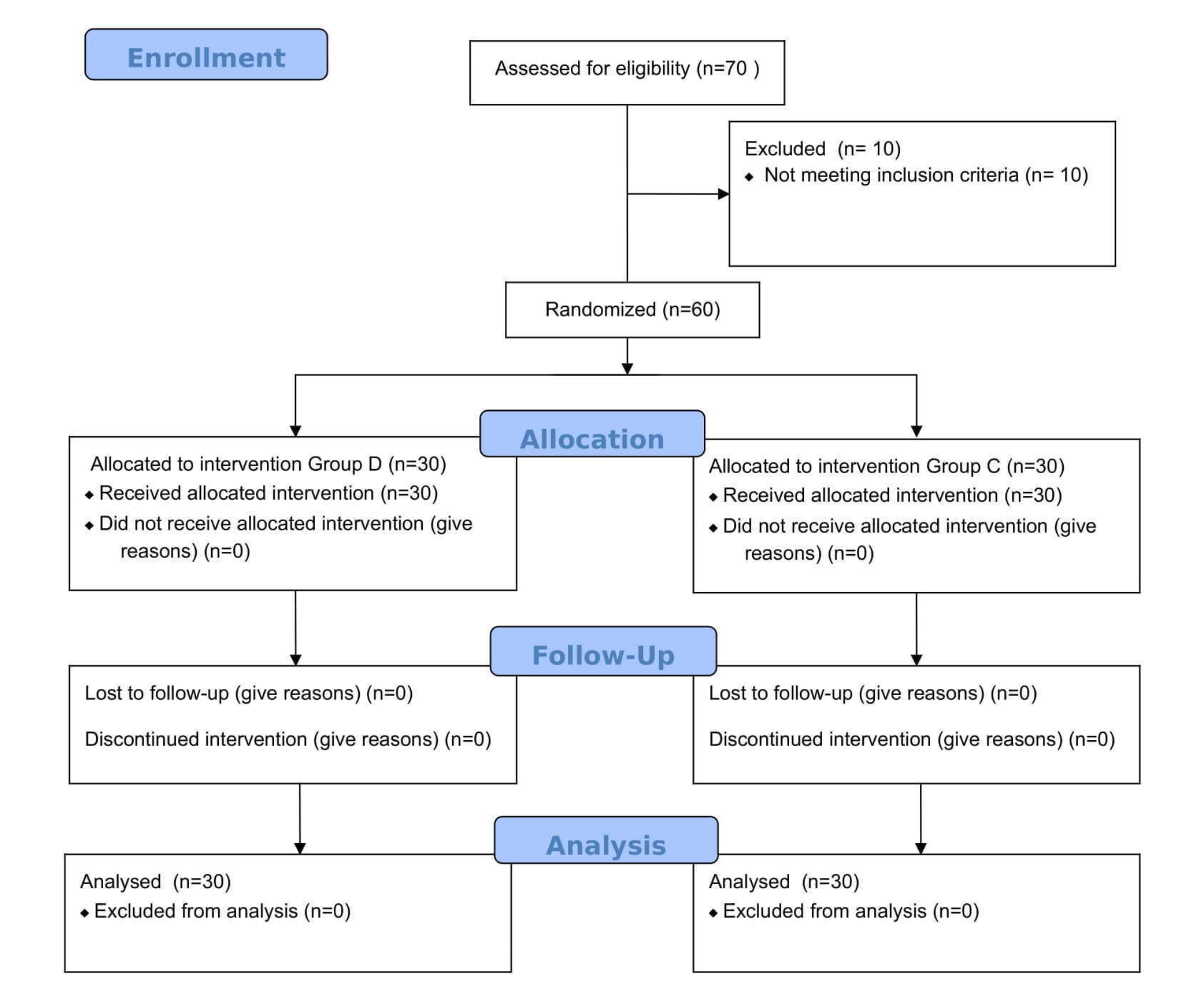
This randomized, double-blinded controlled trial was conducted at Assiut University Hospital after ethical approval from our local committee (No IRB300364), the study was registered on clinical trial registration (NCT04631822) in October 2020. This trial follows CONSORT guidelines and the Declaration of Helsinki. The study was designed to compare the effects of the addition of dexmedetomidine and dexamethasone to bupivacaine on pain control after ACL reconstruction. However, due to a lack of dexmedetomidine supply after starting the study, this group was terminated, and rerandomization was performed at a 1:1 ratio (Fig. 1). Ninety patients, from January 2021 to December 2023, completed the study. Patients were randomly allocated using computer generated random blocks of 10 at 1:1 ratio into two groups:
G I (dexamethasone group): Forty-five patients received a 20 ml mixture of 0.25% bupivacaine and 8 mg dexamethasone (2 ml) injected into the adductor canal under ultrasound guidance at the end of surgery.
G II (control group): Forty-five patients received 20 ml of a mixture of 0.25% bupivacaine and 2 ml of normal saline injected at the adductor canal under ultrasound guidance at the end of surgery. The group assignments were kept in a sealed opaque envelope that opened on the morning of surgery at our local research pharmacy. The drug mixture was prepared by a pharmacist under septic conditions in opaque vials labeled by patient number and research medication. Patients, the data collector and the anesthetist responsible for the block were blinded to the nature of the research mixture. Adult patients aged between 19 and 60 years of both sex and American Society of Anesthesiologists (ASA) physical status I or II were included in the study after providing written informed consent. Patients who refused to consent or withdraw after initial consent, were ASA III or IV, experienced continuous preexisting pain, had known contraindications to peripheral nerve block, including local skin infections, bleeding diathesis, and coagulopathy, were excluded from the study.
Fig. 1
The primary outcome was the dynamic visual analog score (DVAS) 1 month after ACL reconstruction. The secondary outcomes included the postoperative VAS score at 24 h, DVAS score at 2 months and 3 months, time to first analgesic request, and opioid consumption during the first 24 h postoperative and subsequent three months postoperative.
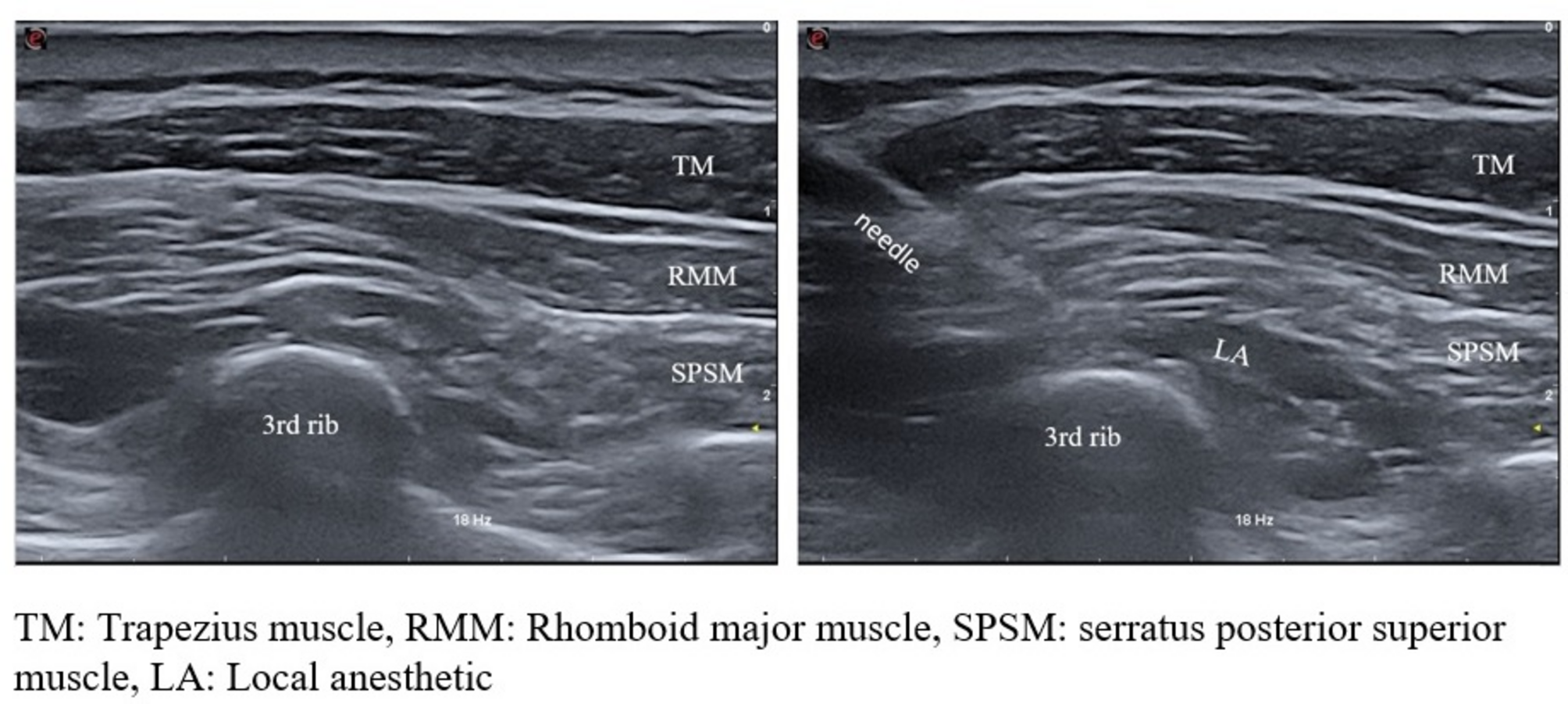
InterventionACL reconstruction was performed under spinal anesthesia. At the end of surgery, sterilization of the thigh was performed. A high-frequency (L6-12HZ) linear ultrasound transducer (GE machine- logic F6 model-Italy) was placed transverse to the longitudinal axis at the mid-thigh level, at a distance halfway between the iliac spine and the patella. The femoral artery was identified underneath the sartorius muscle with the vein just underneath the artery. At this position, the saphenous nerve was placed lateral to the artery in the adductor canal. A single shot nerve block echogenic needle was inserted in plane from the lateral side of the transducer through the sartorius muscle with the tip placed lateral to the artery. Twenty milliliters of 0.25% bupivacaine mixed with either dexamethasone or saline was injected to expand the canal.
MeasuresIn the first 24 h postoperative the measured data were the mean VAS score at 2, 6, 12, and 24 h, time to first analgesic request and total opioid consumption. In the next three months after surgery, both the DVAS and the total amount of codeine consumed per day were evaluated at the first, the second and the third month postoperative.
The rescue analgesia in the first 24 h was paracetamol 1 gm if the VAS score was less than 4 and tramadol 50 mg if the VAS score was more than 4. The regimen for postoperative pain ,at home after hospital discharge, was Solpadine, Smithkline Beecham S.A. Spain, (500 mg paracetamol + 8 mg codeine + 50 caffeine) 4 to 6 times daily as needed, with gradual withdrawal starting from the 7th postoperative day and replacement with 400 mg ibuprofen after telephone consultation with the pain physician responsible for data collection. Postoperative visits to the pain clinic were scheduled for participants at 1, 2 and 3 months postoperative. The telephone number of all participants was taken, and if they skipped the scheduled visit, they were telephoned by the data collector.
Sample sizeAccording to a previous study [15], the mean VAS score for persistent pain after ACL reconstruction was 1.6 at the 6th week after surgery, and the standard deviation (SD) was ± 1.1. A total of eighty patients (40 patients in each group) were needed to detect a 50% reduction in the VAS score between the groups 1 month after surgery, with 90% power and an alpha error of 0.05. To compensate for dropouts, we included ninety patients.
Statistical analysisIBM SPSS software version 22.0 (SPSS Inc., Chicago, IL) was used. The data are presented as the means ± SDs, medians (ranges) and numbers (%) as appropriate. Independent t tests were used to compare means between parametric data. Mann‒Whitney tests were used to compare nonparametric values in the studied groups, and repeated measures analysis will be used for repeated data (blood pressure, heart rate, and visual analog scale (VAS) scores and codeine consumption). The chi-square test or Fisher’s exact test will be used for categorical data. A P value > 0.05 was considered statistically significant.
Comments (0)