This study contributes to the literature by being among the first to examine in detail the impact of a family HHT on health anxiety and related attitudes. By investigating the attitudes toward hypertension prevention in individuals with and without a familial risk of hypertension, this study primarily aimed to examine the impact of health anxiety on these attitudes, while also seeking to identify the effect of demographic characteristics and family history as a secondary objective.
The educational background of participants suggests a generally high level of health literacy, which is known to positively affect disease perception and health attitudes [18, 26]. Furthermore, the presence of financial strain among a portion of participants highlights the potential influence of socioeconomic status on individuals’ ability to engage in preventive health behaviours. This result aligns with the data reported by Schutte et al. [6] that the highest mortality rates standardized by income level and age in 2019 were in low-middle income and low-income countries [6]. Particularly in Turkey, a low-income country in the Middle East, these risks are also relevant to us, and this is believed to increase the pressure on our healthcare system. Uncontrolled hypertension and other health problems thus pose a major threat to public health and are considered a source of understandable concern.
45.2% of the participants reported a family HHT. This rate is higher than the 31.2% family history reported by Arslantaş et al. [13]. Similarly, a study by Kanuda et al. (2018) on hypertension awareness reported a family history rate of 48.2% [14]. Shah et al. [27], in a study investigating a family HHT in Abu Dhabi, found that 2.9% of children had a family HHT [28]. These results suggest that genetic factors are more prevalent in certain communities. Additionally, differences in our study's results may be attributed to the participants' demographic characteristics, socioeconomic conditions, and regional factors.
In Table 2, the prevention and control scores (31.55 ± 7.28) in the subdimensions of the family ASPH indicate high awareness among individuals regarding hypertension prevention. A study by Paulose et al. [29] in southern Ethiopia found that individuals exhibited moderate attitudes toward controlling and preventing hypertension. However, disease and risk knowledge remained lower at 62.7% [27], as in this study, indicating gaps in understanding hypertension risk factors and effects within our country. Thus, it is evident that more informative content on hypertension risks is needed in public health programs.
In controlling hypertension, lifestyle modifications such as dietary changes, reducing alcohol consumption, quitting smoking, and aerobic exercise have now broadened to include less obvious strategies like stress reduction, isometric exercise, and reducing exposure to air pollution [29]. In this study, it is notable that individuals scored average on mental state, physical activity, and nutritional attitude scales. Ma et al. reported that only 32.3% of hypertension patients engaged in physical activity, with emotional stability maintained in only 3.1% and a sad mood in 10.9% [30]. In a 2017 study by Son et al., 15.8% of hypertensive patients who did not engage in regular physical activity experienced depressive symptoms. Zhu and Wang (2024) demonstrated that individuals who eat healthily and stay physically active have a 25% lower likelihood of developing hypertension compared to those with unhealthy diets and inactive lifestyles [31]. Additionally, in this study, high scores in lifestyle and habit factors were observed, with a healthy weight and diet respectively reducing the risk of hypertension by 54% and 28% [32], making these results encouraging. Although the ASPH total score (98.31 ± 21.91) was high, physical activity and mental state are often overlooked in hypertension management, indicating a need for increased awareness and educational efforts in these areas [23].
Health anxiety concerning HAS total (13.75 ± 6.81) was low, suggesting that participants generally showed low sensitivity to physical symptoms and did not experience excessive anxiety. Compared to Bulut and Bozo's (2022) study, health anxiety and greater sensitivity to physical symptoms were reported in individuals with chronic diseases [33]. However, the low anxiety level of individuals in their study may be attributed to factors such as the variability of health awareness and risk perception of different sample groups and the fact that the patient group was not diagnosed with hypertension. Furthermore, very low scores for HAS-2 (3.50 ± 2.34) suggest that individuals are less concerned about the long-term effects of hypertension. This contrasts with the results of Havill et al. [21] and suggests that there is a need for awareness-raising by nurses regarding long-term outcomes.
The overall hypertension control rate is lower among young adults compared to middle-aged or elderly adults [34]. In the correlation analysis conducted, age was significantly associated with some subdimensions of hypertension attitude. A positive correlation was found between age and mental state and physical activity (p = 0.026) and age and nutritional behavior (p = 0.041), indicating that older individuals tend to adopt more active and health-conscious behaviors. Additionally, BMI showed a positive correlation with total attitude (p = 0.006), indicating that individuals with higher BMI scores may exhibit stronger hypertension-related attitudes. This suggests that individuals with a higher BMI might be more conscious of hypertension risks and adopt more proactive attitudes toward disease prevention and management. However, in the regression analysis, men were shown to have lower hypertension attitude scores than women, indicating that women demonstrate higher awareness and more cautious attitudes toward hypertension. The higher awareness of hypertension in women and their more cautious attitudes may be due to their greater sensitivity to health risks, as frequently mentioned in the literature. Similarly, Zhang and Moran (2017) found that individuals aged 18-39 exhibited lower attitudes toward hypertension compared to those aged 40 and above, with young women displaying higher hypertension awareness than men in that age range [34]. Conversely, in a study by Gong et al. [35], age was identified as an important factor in attitudes toward hypertension, showing that younger individuals exhibited more positive attitudes [36]. However, no significant difference was found between men and women regarding hypertension attitude. These differences in results may be attributed to cultural, socioeconomic, and geographic variations. Particularly, societal health perceptions and access to healthcare services can impact individuals’ attitudes toward chronic conditions like hypertension. This may explain why men are less likely to seek healthcare services and pay less attention to health-related matters [37].
It is often noted that women are more conscious than men in matters related to diet and health behaviors, which plays a significant role in managing chronic diseases such as hypertension [38, 39]. The regression analysis showed that gender had a significant effect on nutritional attitudes (B = −0.685, p ≤ 0.001), consistent with the literature[34, 40, 41]. The lower nutritional attitudes among men may stem from a lower level of motivation or awareness in adopting healthy eating habits [42]. Furthermore, demographic factors such as marital status, educational level, and income level did not significantly impact hypertension attitudes, suggesting that these variables do not strongly influence hypertension attitudes. Effective hypertension management generally involves individuals consciously taking preventive and control measures [43]. The literature also supports that prevention and control strategies are critical in managing hypertension [14, 35, 43]. It is also believed that the prevention and control of hypertension are associated with lifestyle factors [29]. In our model, the high constant coefficient for habits and lifestyle (Table 4) reflects changes in hypertension attitude. Similarly, Perdita et al. [44] identified a link between lifestyle habits and hypertension awareness among the adult population [45]. The high constant coefficient for habits and lifestyle in our model suggests that lifestyle factors significantly impact hypertension attitudes. Nursing care plays a crucial role in assisting individuals to adopt these lifestyle changes, encouraging healthy habits, and providing effective strategies for hypertension management. This result is supported in the literature by studies emphasizing the interconnectedness of lifestyle and hypertension prevention strategies [43, 45], indicating that lifestyle changes and preventive health behaviors are essential in managing hypertension.
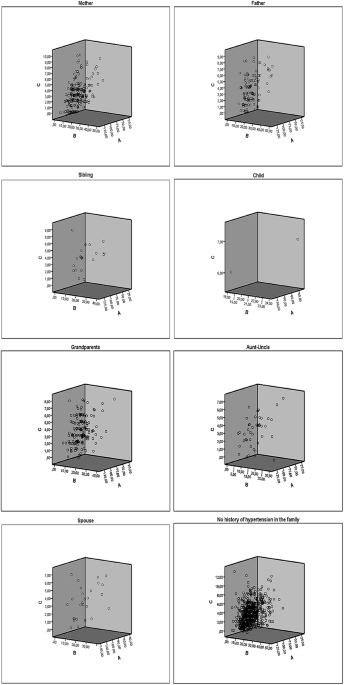
Table 4 The impact of independent variables on ASPH total: regression analysis results.Although an overall negative association was observed between family HHT and attitudes toward hypertension prevention, subgroup analyses revealed that individuals with hypertensive parents or siblings exhibited more favourable attitudes, as indicated by their ASPH scores. These findings suggest that close familial ties may enhance individuals’ health awareness and concern regarding hypertension. Furthermore, regression analyses identified both family HHT and gender as significant predictors of hypertension-related attitudes. Notably, men demonstrated lower levels of awareness and less engagement in preventive behaviors, which is consistent with previous research [28, 46, 47]. However, a study conducted in Sudan reported low disease awareness among those with a family HHT, indicating the potential moderating role of sociocultural and demographic factors [48]. Moreover, individuals with hypertensive spouses or children reported higher anxiety and stronger disease-related attitudes (see Fig. 1), possibly due to emotional closeness and perceived vulnerability. In support of this, Kubb and Foran [49] found that health anxiety is often shared within families, with a significant correlation between anxiety levels for spouses and children. Expanding on subgroup-level findings, the regression analysis supported a similar pattern in the habits and lifestyle subdimension of hypertension attitudes. Gender appeared to have a stronger negative impact on this subdimension compared to family HHT. In this study, individuals with hypertensive spouses demonstrated higher anxiety and stronger disease-related attitudes, consistent with Hu’s (2022) hypothesis that social and emotional bonds amplify disease perception [50]. This finding may be explained by the perception of illness as a personal threat due to the closeness and interdependence of the spousal relationship. For individuals with hypertensive children, attitudes and anxiety levels varied more widely. This heterogeneity may reflect how parental concerns differ individually, leading to varied emotional responses and perceptions. Similarly, participants with hypertensive grandparents showed more variable attitudes. This is consistent with Priboi et al. (2016), who noted that grandparents often view themselves as emotional anchors in the family, prioritizing the well-being of others over their own [51].
In a study by Wakefield et al. (2014) with the grandparents of children with cancer, it was similarly shown that these individuals minimized their emotional and physical needs in order to stay strong for their families [22]. These results may be explained by elderly individuals’ insufficient sharing of health information within the family or a decline in health awareness over time, which can prevent the transmission of this knowledge to their grandchildren. In the study by Havill et al. [21], it was shown that living with a sibling who has a chronic illness can cause health anxiety in healthy siblings, leading them to worry about their own health. Compared to that study, individuals with a family HHT in their siblings were observed to have moderate levels of anxiety and attitudes toward their own health in our study. According to Havill’s results, individuals might be expected to feel more anxiety regarding their health, while the present study indicates that their attitudes toward hypertension are more balanced and less extreme [21]. This suggests that, unlike other chronic illnesses, hypertension may result in a more balanced level of concern regarding one’s health, or that individuals, despite being aware of the adverse effects of the disease, may not exhibit HAS total. In Herrera et al.’s [42] study, it was shown that pushing individuals with chronic conditions such as diabetes and hypertension to comply with treatment, through pressure and comparison (using an aunt as an example), had adverse effects [52].
In a quantitative study by Bulut and Bozo [34] on individuals with health anxiety, the loss of a cousin due to cancer and the recurrence of an aunt’s illness were identified as significant predictors of elevated health anxiety levels. Unresolved loss issues, particularly, were central to participants' health anxiety and showed indications of hypochondriasis [33]. In this study, however, individuals with an aunt, uncle, or other extended family members with a history of illness showed a more scattered pattern in their health attitudes compared to those with immediate family members. This suggests that the health history of more distant relatives may have a more indirect and ambiguous effect on the individual. While the health history of close relatives, such as a parent or sibling, tends to result in more pronounced changes in health attitudes, a history of hypertension in more distant relatives, such as an aunt or uncle, did not lead to clear attitudes in the individual. This result indicates that the influence of family members may vary depending on their closeness and that a history of illness in distant relatives may lead to more complex attitudes. Examining Fig. 1, it is suggested that a family HHT intensifies individuals’ awareness and attitudes toward hypertension, while those without such a history may hold a broader and more varied perception. Additionally, although our regression analysis did not reveal a direct effect of HAS total and HAS-2 on ASPH, Fig. 1 suggests a relationship between family HHT and both HAS total and HAS-2 scores. This suggests that, indirectly, increased health anxiety in individuals with a family HHT may influence their hypertension attitudes. The finding that a family history of close relatives with hypertension leads to significant changes in anxiety and attitudes, whereas more distant relatives’ histories have a more ambiguous effect, offers a new perspective in the fields of internal medicine, public health, and nursing care.


Comments (0)