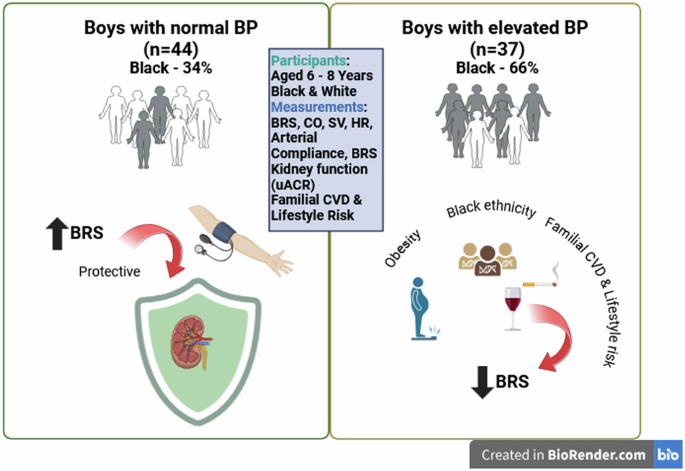
The aim of our study was to investigate the relationship between BRS (as an autonomic marker of blood pressure regulation) and kidney function in preadolescent boys with and without elevated blood pressure, while considering markers of adiposity and familial cardiovascular-and lifestyle risk. In boys with normal blood pressure, we found a protective association between BRS and uACR, but in boys with elevated blood pressure, BRS was associated with BMI and a positive family history of cardiovascular-and lifestyle risk.
In the early phases of primary hypertension, a hyperkinetic state is often indicated [20]. Increased sympathetic activity leads to an elevated heart rate and subsequently augmented stroke volume and cardiac output [20]. Our findings showed BRS, and other cardiovascular measures were comparable between boys with normal and elevated blood pressure. After adjusting for BMIz and race, the resting heart rate of the boys with elevated blood pressure were significantly higher, yet BRS, stroke volume and cardiac output remained comparable. A possible explanation for this finding is that our study sample consisted of young, healthy school children with blood pressure reported as a single measure at one time-point. Delimitation was based on elevated BP indicated when participants are stratified within the 90th percentile and not necessarily hypertensive [19]. Therefore, in the boys with elevated blood pressure, pertinent autonomic imbalance in favour of sympathetic activity may not be evident yet, to a degree where a notable BRS difference could be seen. Despite the absence of significant observed differences in BRS and other cardiovascular measures, we persisted with further analysis based on the assumption that in the presence of elevated blood pressure an altered relationship between baroreceptor sensitivity and kidney function may already be indicated.
A shift in autonomic tone in favour of sympathetic activity, also pertains to kidney function in children. Rutigliano et al. suggested microalbuminuria as marker of autonomic imbalance based on glomerular hyperfiltration associating with sympathetic hyperactivity in a paediatric cohort [6]. Our findings in boys with normal blood pressure indicated a negative association between BRS and uACR possibly indicating the effective regulation of cardiovascular and renal function by the autonomic nervous system. Therefore, through efficient baroreflex control, blood pressure is adequately regulated, and renal damage is prevented preventing subsequent urinary leakage of albumin. Conversely so, the absence of this finding in boys with elevated blood pressure may hypothetically be an indication of the possible impairment of adequate blood pressure and kidney function modulation by the autonomic nervous system.
It is important to consider established risk such as adiposity and familial history, significantly contributing to childhood hypertension and possibly accompanying autonomic imbalance and inevitably affecting kidney function. Increased adiposity in children may negatively affect autonomic balance, shifting in favour of sympathetic activity and therefore adjusting blood pressure control [21]. Rutigliano et al. found altered autonomic function in children with high metabolic risk (obese or type 1 diabetic) [6]. Particularly in obese participants, greater blood pressure variability with postural change pointed to early BRS dysfunction. A study within this cohort by Mokwatsi et al. showed low incidence of obesity [22]. Irrespective of this, in our study the BMIz-score independently and inversely associated with BRS in the group with elevated blood pressure. This may indicate that with increase in body mass, an early shift in autonomic nervous system balance may occur, favouring increased sympathetic tone and modulation. This observation is additionally supported by the higher resting heart rate observed in this group.
Another factor that warrants consideration is the heritability of CVD risk factors whilst also considering parental lifestyle risk. The role of family history in contributing to CVD risk is underscored by our findings, which align with those of Mathews et al. [7] who reported that lower baroreflex sensitivity (BRS) associated with a familial predisposition to CVD. This may be due to epigenetic factors [12], environmentally influenced and eventually inherited mechanisms, which can amplify susceptibility to CVD by altering gene expression patterns associated with autonomic and cardiovascular regulation. These combined effects may have significant implications for blood pressure regulation and kidney function, potentially increasing susceptibility to CVD-related complications later in life.
Furthermore, our findings are also in alignment with previous studies who postulated earlier onset of vascular changes and affected blood pressure in Black paediatric cohorts [23]. This was however not the focus of our study but remains a significant factor to consider when evaluating early changes in autonomic regulation, blood pressure and hence kidney function in a South African context.
Consequently, the findings of our study emphasize in children the importance of considering autonomic regulation, adiposity, race and familial risk factors to possibly mitigate early shifts in autonomic balance and reduce long-term risks of hypertension, kidney dysfunction, and cardiovascular complications possibly later tracking into adulthood.
It is important to consider findings in the light of the studies’ strengths and limitations. A strength of this study is the inclusion of healthy young boys which allowed assessment of early life markers of cardiovascular and renal function. Furthermore, by including only boys this study tried to control for sex-based physiological differences. A limitation of this study was the cross-sectional observational design which prevents generalization to the broader population and no definitive cause-and-effect conclusion can be drawn. Furthermore, the classification of blood pressure was based on a once-off visit only. Hypertension diagnoses in paediatric cohorts can only be verified as guidelines specify with BP measured at three different time-points [19]. The authors also acknowledge the limitation of not considering dietary data and physical activity in the statistical models as these parameters were not included in the data collection of the main study. Another limitation to be noted is the reliance of a first-morning voided urine sample to determine uACR. We acknowledge that a 24-h urine collection would have been a better representation of daily urinary albumin and creatinine excretion, however, the implementation thereof in a paediatric cohort poses a logistic and compliance challenge. Result interpretation must be with caution due to the relatively small groups observed. Therefore, the small effect size could limit the magnitude of physiological interpretation.


Comments (0)