
Remember me
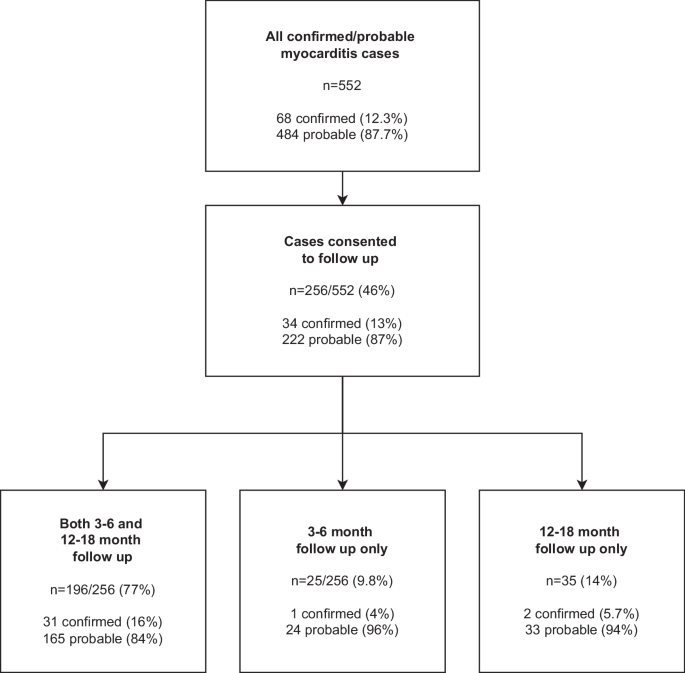
There were 552 cases of myocarditis (68 (12%) confirmed and 484 (88%) probable cases as classified by the U.S CDC case definition (Supplementary Table 1)14 identified in Adverse events following immunisation (AEFI) reports to Australia’s national regulatory agency, the Therapeutic Goods Administration (TGA) between February 2021 and July 2022 (Fig. 1).
Fig. 1
Study population and follow up recruitment.
Demographic and clinical data at presentation (n = 552)Of the 552 cases, 487 (88%) were following Pfizer–BioNTech BNT162b2 and 65 (12%) following Moderna mRNA-1273, equating to a rate of 1.2 cases per 100,000 Pfizer–BioNTech BNT162b2 doses and 1.4 cases per 100,000 Moderna mRNA-1273 doses administered. Most myocarditis cases occurred after administration of dose 2 (70%), with fewer cases occurring after dose 1 (20%) and dose 3 (9.4%). The median age was 22 years [interquartile range IQR 17–33, range 5–76 years]. There were three times as many male cases as female cases (76% male vs 24% female) (Table 1). There was no difference in age, sex or Indigenous status when comparing confirmed with probable cases (Supplementary Table 2)
Table 1 Demographics, past medical history, clinical and diagnostic findings of initial presentation in 552 confirmed and probable myocarditis cases following mRNA COVID-19 vaccination presenting between 21 April 2021 and 5 July 2022, comparing cases who participated in any follow up and those who did notAcute clinical courseMost cases presented within 7 days (84%) of their COVID-19 vaccine (median time to onset: 3 days [IQR 1–4]), with no difference in timing between confirmed and probable cases. The most common presenting symptom was chest pain/pressure/discomfort (96%) followed by shortness of breath (34%) (Table 1). Confirmed cases were more likely to have pleuritic chest pain (28% vs 12%) and fever (22% vs 12%) compared to probable cases (Supplementary Table 2).
Most individuals were hospitalised (86%) with a median length of hospital stay of 2 days [IQR 2-3]. Twenty cases (3.7%) required intensive care unit (ICU) admission, with two individuals requiring intubation and mechanical ventilation and one requiring extracorporeal membrane oxygenation. Twelve individuals (3%) (10 males (83%) and 2 females (17%), median age 41 years [IQR: 25-49]) reported having procedures or surgery during their admission. There were nine (75%) cardiac procedures; eight coronary angiography/catheterisation and one pericardiocentesis. There were three non-cardiac procedures; a cholecystectomy, an arthroscopy and a muscle biopsy for investigation of an alternate aetiology. All hospitalised individuals were discharged home and there were no deaths.
Ongoing symptoms at time of discharge were reported in 27% of cases, mostly with ongoing chest pain. Most individuals (88%) were discharged on anti-inflammatory medication, 53% were advised to restrict physical activity. Confirmed cases had a higher rate of corticosteroid and non-antiarrhythmic medication requirements on discharge and were more likely to be advised of physical restrictions on discharge (Supplementary Table 2).
Diagnostic findingsCardiac magnetic resonance imaging (cMRI) was performed at initial diagnosis for 149 individuals, of which 128 (83%) were abnormal (57/57 (100%) of confirmed and 71/92 (77%) of probable cases). Of those who had cMRIs, the median age was 22 years, and most cases were male (83%) and following dose 2 (71%).
There were three cases with histopathology performed on cardiac biopsies as part of initial assessment, all in males aged 34–53 years and following dose 2 Pfizer–BioNTech BNT162b2. All had prolonged hospitalisations (13–16 days) and two required ICU admission. Two showed lymphocytic infiltrates and evidence of myocyte necrosis and degeneration consistent with lymphocytic myocarditis while the other found no evidence of myocarditis or pericarditis.
Follow up cohort (n = 256)Of the 552 myocarditis cases, 256 (46%) consented to follow up and completed at least one follow up: 221 (86%) completed the 3–6 month follow up survey (median time to follow up 109 days [IQR 96–140]), 231 (90%) completed the 12–18 month follow up survey (median time to follow up 402 days [IQR 385–444]), and 196 (77%) completed both (Fig. 1).
Follow-up cases were aged 7–76 years with the median age higher in those who consented for follow-up than those who did not (24 [IQR 17–37] years vs 20 [IQR 17–29] years, P < 0.05). There was a higher proportion of cases with a family history of cardiac conditions of interest (sudden cardiac death, cardiomyopathy, permanent pacemaker and/or implantable cardioverter defibrillator or cardiac adverse event to any previous vaccine), but a lower proportion of past medical conditions in the follow-up group compared to the no follow-up group. There was no sex difference or difference in proportion of Aboriginal and Torres Strait Islanders participating in follow-up. Individuals who had follow-up had higher rates of syncope, dizziness, headache, and lethargy compared to individuals who did not have follow-up. They also had more severe disease with a higher proportion of individuals requiring ICU admission (6% vs 1.8%) and reporting ongoing symptoms (48% vs 8.1%) and exercise restrictions (66% vs 42%) at discharge (Table 1).
Clinical progressionThe proportion of individuals who had follow-up and reported ongoing symptoms was 48% (123/256) at discharge, 60% (133/221) at 3–6 months, and 35% (81/231) at 12–18 months (Table 2). Chest pain, heart palpitations, and shortness of breath were the most reported symptoms (Table 2, Fig. 2a). While there was no difference in the proportion of males and females reporting ongoing symptoms at discharge or at 3–6 months, there was a significantly higher proportion of females reporting ongoing symptoms at 12–18 months compared to males. There was a higher proportion of females reporting palpitations at all time points, lethargy/fatigue at both follow-up time points, and shortness of breath at 12–18 months compared to males. Ongoing symptoms at 12–18 months was also associated with older age (Table 3).
Fig. 2: Ongoing symptoms in myocarditis following a COVID-19 mRNA vaccine.
A Cases who completed any follow-up: discharge (n = 256), 3-6 months (n = 221) and 12-18months (n = 231). B Cases who completed all follow-up timepoints (n = 196).
Table 2 Clinical features in 256 cases of myocarditis following a COVID-19 mRNA vaccine who participated in follow-up, at discharge following initial diagnosis, 3–6 months and 12–18 months following initial diagnosis and by sexTable 3 Clinical progression and self-assessment of health-related quality of life on EuroQol 5-dimension, 5-level (EQ-5D-5L) and overall health on EuroQol Visual Analogue Scale (EQ-VAS) among myocarditis cases following mRNA COVID-19 vaccination at 3–6 and 12–18 months, by ongoing symptoms reported at follow upThe proportion of individuals requiring medication decreased from 92% (235/256) at discharge to 13% (31/231) at 12–18 months, which included 9% (20/231) on anti-inflammatories, 7% (16/231) on other cardiac medications including antihypertensives and beta-blockers, and none on anti-arrhythmic medication. Restrictions on exercise/physical activity decreased from 66% (168/256) at discharge (all clinician recommended) to 8% (19/231) at 12-18 months (all self-initiated). Hospital representation decreased from 27% (60/221) at 3–6 months to 20% (47/231) at 12–18 months; with 18% (41/231) to emergency department, 5.6% (13/231) hospital admission, and 1.3% (3/231) ICU admission at 12-18 months (Table 2). No individual required surgical intervention or additional procedures relating to their myocarditis diagnosis, during the follow up period. There were no deaths reported. Females were more likely to have hospital representations and remain on medications (Table 2).
After adjusting for age and sex, individuals with ongoing symptoms had higher odds of ongoing medication requirements, physical activity restrictions, and hospital representation at both 3-6 months (adjusted odds ratio aOR 3.52 (95% CI: 1.62–7.67), 6.13 (95% CI 2.84–13.24), 2.01 (95% CI 0.89-4.51 respectively) and 12–18 months (aOR 8.02 (95% CI: 2.62–24.55), 37.47 (95% CI: 4.48–313.18), 2.19 (95% CI: 0.98–4.90) respectively) compared to those without ongoing symptoms (Table 3).
Following clinical review and on clinician recommendation, 53 cases (22.9%) had another COVID-19 vaccination in the follow up period (median time to revaccination 166 days [IQR 121-207 days]); 19 Astrazeneca ChAdOx1-S (AZD1222), 8 Pfizer–BioNTech BNT162b2 and 26 Novavax NVX-CoV2373, all of whom were asymptomatic at the time of revaccination. Females were more likely to receive another COVID-19 vaccination (Table 2). Eight individuals reported self-resolving cardiorespiratory symptoms on revaccination (four following Astrazeneca ChAdOx1-S and four following Novavax NVX-CoV2373, all as their second COVID-19 vaccine dose). All sought medical review and investigation of myocarditis following subsequent vaccination, with no evidence or diagnosis of myocarditis recurrence found.
As not all individuals completed follow-up at both timepoints, the progression of symptoms, exercise restrictions, medications, re-presentations, and further COVID-19 vaccinations by sex and age was examined in 196 (77%) cases who completed both follow-up timepoints (Fig. 2b, Fig. 3). In this subset, there was an increased proportion of individuals reporting symptoms at 3-6 months compared to discharge following initial diagnosis (Fig. 2b and Fig. 3), though the proportion reporting symptoms at 12-18 months was similar to that of the larger group (Fig. 2b vs Fig. 2a). Individuals in the older age groups were more likely to have ongoing symptoms and ongoing medication requirements. Those aged <24 years had the highest hospital re-presentation rates at 3-6 months, mostly to emergency departments only, but by 12-18 months, they had the lowest rate of ongoing symptoms, exercise restrictions, and medication requirements (Fig. 3).
Fig. 3
Progression of symptoms, exercise restrictions, medications, re-presentations and further COVID-19 vaccinations by sex and age, in myocarditis cases following mRNA COVID-19 vaccination who completed both 3-6 and 12-18 month follow up (n = 196).
Quality of lifeEuroQol 5-dimension, 5-level (EQ-5D-5L) questionnaire and EuroQol Visual Analog Scale (EQ-VAS) was completed at both follow-up timepoints in 83% (152/183) of individuals aged 18 and over. In this subset of individuals, the proportion reporting problems decreased in all domains over time; from 16% at 3–6 months to 6% at 12–18 months for problems with mobility, from 6% to 2.0% for self-care, from 41% to 20% with performing usual activities, from 57% to 25% with pain/discomfort, and from 60% to 33% with feeling anxious or depressed (Fig. 4A). Of those who reported problems, most were slight to moderate in severity (Supplementary Fig. 1). As there was no baseline EQ-5D-5L data on cases prior to their diagnosis nor a control group, EQ-5D-5L data from the Australian population surveyed in July 202118 is included for comparison (Fig. 4A).
Fig. 4: Self-assessment of health-related quality of life among myocarditis cases following mRNA COVID-19 vaccination who completed EuroQol 5-dimension, 5-level (EQ-5D-5L) questionnaire at both 3–6 and 12–18 month follow up (n = 152).
A Health-related quality of life. B Weighted quality of life measure. C Self-assessed overall health.
Overall, individuals reported having good health which improved with time; EQ-5D index increased from 0.92 [IQR 0.80–0.97] at 3–6 months to 1.00 [0.94–1.00] at 12–18 months. However, individuals with ongoing symptoms had significantly lower EQ-5D-5L index scores and higher odds of reporting problems across all 5 domains at both timepoints after adjusting for age and gender (Table 3, Fig. 4B).
Overall, individuals reported having good health with a median overall health status (EQ-VAS) score of 70 [IQR 50–80] at 3–6 months and improving to 80 [IQR 70–90] at 12–18 months (Fig. 4B). Individuals reporting ongoing symptoms had significantly lower EQ-VAS compared to those without symptoms (65 [IQR 49–75] vs. 80 [IQR 75–91] at 3-6 months, 75 [IQR 60–84] vs 85 [IQR 77–93] at 12–18 months) (Table 3, Fig. 4C).
Comments (0)