Clinical trial
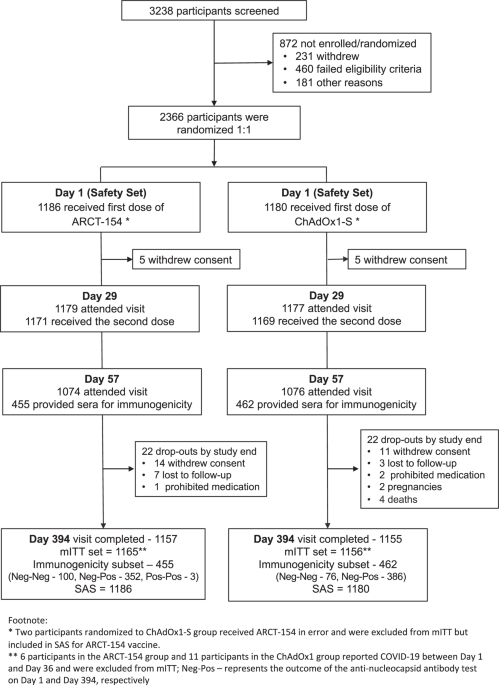
VAT00001 was a Phase I/II randomized, modified double-blind, placebo-controlled, first-in-human, dose-escalation trial. The trial design and interim results have been described in the prior publication26. In brief, participants were healthy volunteers without prior exposure to SARS-CoV-2, stratified by age (18–49 years of age, 50 and above). The vaccine formulations evaluated included one or two dose levels (1.3 or 2.6 μg) of a recombinant protein vaccine comprising the stabilized prefusion spike of the ancestral (WA-1) SARS-CoV-2 strain, delivered with AS03 (GSK) or AF03 (Sanofi) adjuvant or without adjuvant. The dosing schedules evaluated included a single administration (D01) or two doses separated by a 21-day interval (D01, D22).
Assay methods
The microneutralization assay (Global Clinical Immunology, Sanofi Vaccines, Swiftwater, PA) and GCN-4 binding antibody enzyme-linked immunosorbent assay (ELISA; Nexelis, Laval, QC) methods have been described elsewhere26,27. Blood samples obtained at baseline and post-vaccination (D01, D22, D36) were assessed in the above assays.
A qualified Binding Antibody Multiplex Assay (BAMA) was used to detect endemic coronavirus-specific IgG in serum from participants at baseline (D01) in the VAT00001 trial. The assay detects antibodies to the receptor binding domain (RBD) and to full-length spike of endemic human coronaviruses HKU1, 229E, NL63, and OC43. Both forms of CoV antigens were chosen since RBD exhibits lower homology across CoVs, whereas the full-length spike contains regions that are more conserved across CoVs20,28,29. Antigens included in the assay are detailed in Supplementary Table 1. The method for detecting HCoV-specific antibodies, described previously9, includes sample incubation with antigen-coated beads for 30 min (MagPlex beads, Luminex Corporation). NeutrAvidin-coated beads are bound to a biotinylated rabbit anti-6xhis antibody, which then captures His-tagged HCov proteins in BAMA diluent (PBS, 1% milk blotto (w/v), 5% normal goat serum, 0.05% Tween). Samples were tested at a single dilution of 1:100 in assay diluent, then added to the bound beads and then incubated for 30 min on an orbital plate shaker. Human IgG HCoV-specific antibodies are then detected using an anti-human IgG phycoerythrin (PE) labeled detection antibody (Southern Biotech). Plates containing the bound microspheres/antigen/antibody complex are read on a BioPlex 200 instrument to measure fluorescence intensity (FI). Duplicate wells are averaged to provide a mean fluorescence intensity (MFI) value. Background binding (no sample and no antigen controls) is subtracted from each sample well (Net MFI), which is then used for statistical analysis. The dynamic range of the Bioplex instrument is 2.0–4.5 (log10 transformed MFI). Assay controls included a titrated HCoV seropositive plasma sample (HCoV-PC55 plasma, kindly provided by Dr. Paul Goepfert (University of Alabama) and HCoV spike (AB711725 mAb, kindly provided by Dr. Kevin Saunders, Duke Human Vaccine Institute) as outlined in Supplementary Table 1. Additionally, an irrelevant human monoclonal antibody (7B2) was used as a negative control. Additional details regarding the specificity of the assay for endemic HCoV and the 7B2 negative control mAb binding are shown in Supplementary Fig. 1 (A and B), including the non-reactivity of a SARS-CoV-2-specific monoclonal antibody (AB712384 mAb, kindly provided by Drs. Kevin Saunders and Barton Haynes, Duke Human Vaccine Institute) to the endemic HCoV antigens.
The study was done in compliance with the International Conference on Harmonization guidelines for Good Clinical Practice and the principles of the Declaration of Helsinki. The protocol and amendments were approved by the applicable Independent Ethics Committees and Institutional Review Boards and the regulatory agency as per local regulations. Written informed consent was obtained from the participants before any study procedures were done26.
Statistical methods
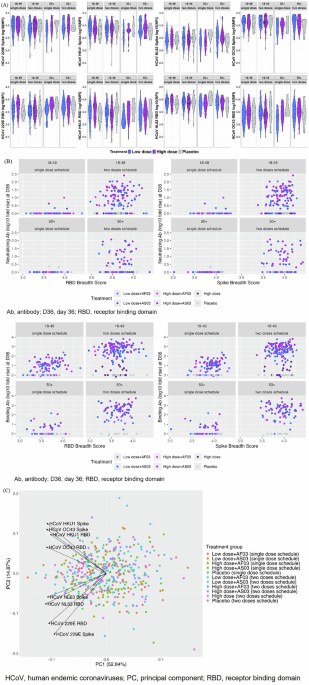
We evaluated the RBD or spike HCoV antibody magnitudes at D01 and vaccine formulation as predictors of the D22 or D36 post-vaccination neutralizing antibody titer or binding antibody concentration using linear regression stratified by age (18–49, 50+) and dosing schedule (single dose, two doses). Additionally, we examined RBD and spike breadth scores as predictors by calculating the mean magnitude of the four HCoV RBDs or four HCoV spike proteins, respectively. Scores were calculated by first averaging the response magnitudes of the four individual antigens within each panel for each sample (i.e., mean of [HKU1, 229E, NL63, and OC43 RBDs] and mean of [HKU1, 229E, NL63, and OC43 spike proteins]). The resultant mean was then log10 transformed for analysis and plotting.
Statistical analyses were conducted using R v4.3.0. Principal component analysis (PCA) was conducted using the R function ‘prcomp,’ and a plot of PC1 and PC2 was generated to visualize potential outliers or clusters and the relationship between those RBD or spike HCoV antibodies plotted using the R package ggfortify. Correlations were evaluated using Spearman’s rank correlation. An alpha level of 0.05 was used to denote statistical significance. P-values were not adjusted for multiple comparisons.

Comments (0)