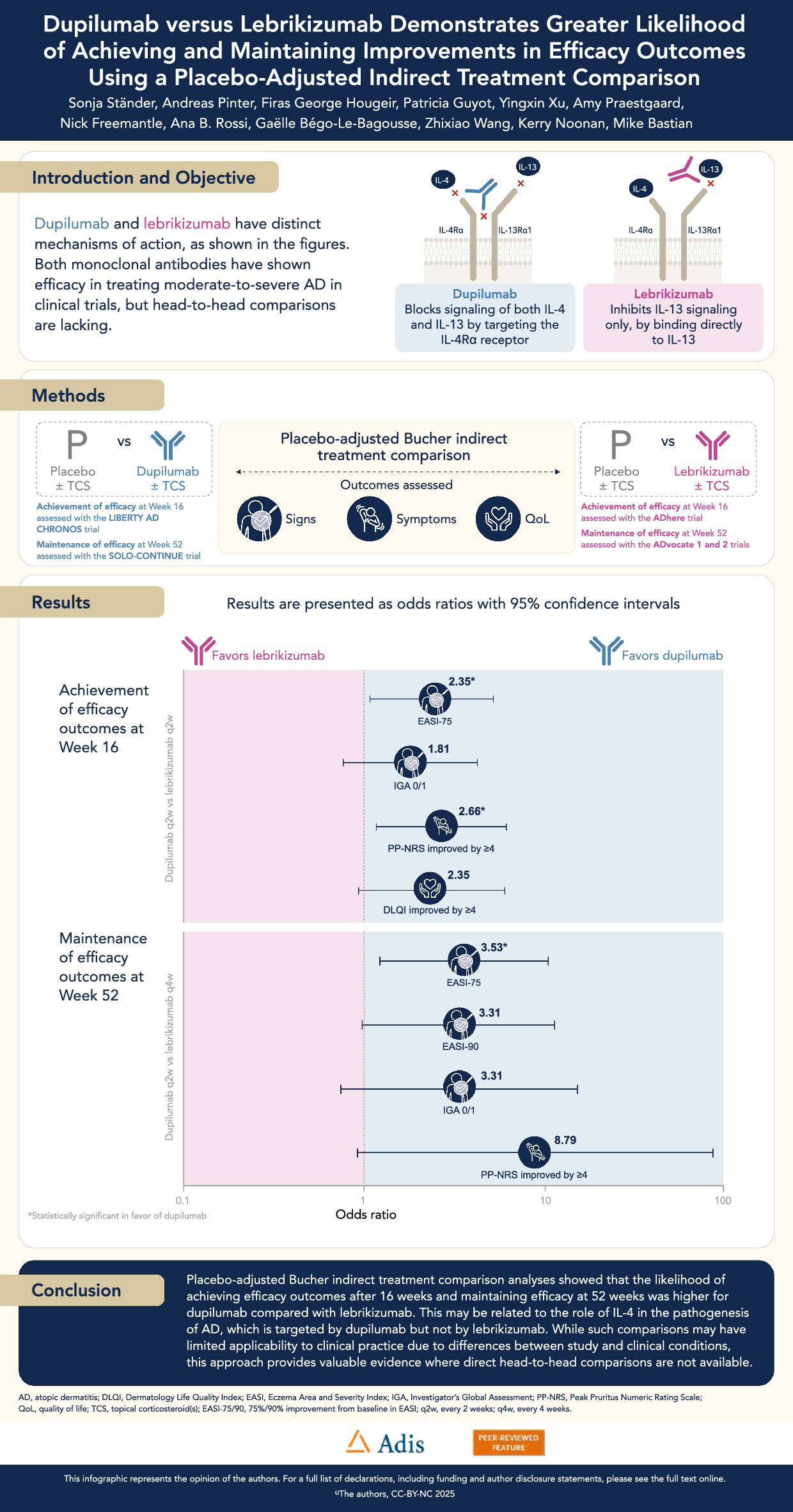
Phase 3 randomized controlled trials have shown that treatment with dupilumab and with lebrikizumab significantly improved signs, symptoms, and QoL compared with placebo. However, there is a lack of head-to-head trials comparing both treatment options. We therefore conducted this placebo-adjusted Bucher ITC analysis of clinical trial data for patients with moderate-to-severe AD. The analysis showed that the likelihood of achieving improvements in AD signs and symptoms, and quality of life, following 16 weeks of treatment, was higher for patients treated with dupilumab plus TCS compared with lebrikizumab plus TCS. Furthermore, the likelihood of maintaining responses in clinical signs and symptoms at week 52 was higher in patients treated with dupilumab q2w compared with lebrikizumab q4w.
In the absence of direct head-to-head treatment comparisons, the most frequently used and most robust ITCs are Bucher ITCs, network meta-analyses (NMAs), and anchored MAICs [17]. Each ITC approach has its own strengths and weaknesses.
A Bucher ITC is an adjusted comparison for aggregate data that can be used to estimate the relative efficacy of two treatments through an indirect comparison with a common comparator [12]. In this case, the common comparator allowing the adjustment is the placebo arm. Bucher ITCs are useful, for example, when there is only one study per pairwise comparison, and have the key advantage that the benefits of randomization are preserved [18]. The importance of preserving the benefits of randomization is highlighted in our analyses because somewhat similar results are achieved in the active treatment groups in each trial, but with higher responses in the placebo groups of the lebrikizumab groups. We observed higher placebo response rates at week 16 in ADhere and at week 52 in the ADvocate 1 and 2 maintenance phase compared with CHRONOS and SOLO-CONTINUE. This difference is particularly notable in the maintenance phase comparison. However, based on the pharmacokinetic profiles of dupilumab and lebrikizumab, neither active substance would be detectable 36 weeks after treatment withdrawal. This pharmacokinetic reality supports our methodological decision to use placebo data as the common comparator in the ITC, as these data provide an unbiased counterfactual estimate of the off-treatment health status in the population of participants recruited to the trials.
NMAs are also placebo-adjusted comparisons allowing for comparison of multiple treatments with a common comparator, usually a placebo arm. Comparisons of dupilumab with other treatments for AD tend to focus on short-term therapy (e.g. ≤ 16 weeks) with Janus kinase inhibitors, and few distinguish patients who received concomitant TCS from those who received only monotherapy [19,20,21,22]. Silverberg et al. [22] performed a Bayesian NMA of studies reporting the efficacy of systemic therapies for moderate-to-severe AD without TCS. The authors reported similar achievement of IGA 0/1, EASI-75, EASI-90, and ≥ 4-point improvement from baseline in PP-NRS between dupilumab and lebrikizumab at week 16. Drucker et al. [20] performed an NMA comparing the efficacy and safety of lebrikizumab with other systemic therapies for AD. While lebrikizumab demonstrated comparable efficacy to dupilumab in continuous outcome measures for patients with AD, the investigators noted that dupilumab showed higher odds of achieving binary efficacy end points. These binary outcomes included EASI-75, EASI-90, and IGA 0/1.
A MAIC is an approach that can further adjust for differences in patient baseline characteristics between studies using individual patient data from one study. MAICs can be anchored (when comparing randomized controlled trials with a common comparator) or unanchored (if a common comparator is not available). Anchored MAICs are performed when there is a common comparator; unanchored MAICs are recognized to be the weakest approach. Organizations including NICE [13] and the ISPOR Task Force [14] recommended only using such an approach if anchored comparisons are not possible. MAICs require access to patient-level data for one of the comparator studies to adjust for the mean baseline data of the comparator, so they are, therefore, not reproducible by researchers without access to these patient-level data. In addition, the selection of the explanatory variables is not a straightforward process. An anchored MAIC should adjust for all potential effect modifiers. However, in practice, selecting these variables involves a combination of literature review, expert opinion, and subgroup analysis of the study with individual patient data. This process requires a balance: including too few variables can lead to a biased estimate, while including too many may overly restrict the effective sample size, sometimes to only a few patients. Exploring the use of two different sets of explanatory variables could provide an opportunity to test the robustness of the results.
Rand et al. [23] conducted an unanchored MAIC, comparing lebrikizumab (ADvocate 1 and 2) with dupilumab (SOLO-CONTINUE), and reported better or comparable efficacy for lebrikizumab; however, the study used an unanchored approach and compared patients treated strictly with dupilumab monotherapy with patients treated with lebrikizumab for whom intermittent topical anti-inflammatory therapy was allowed. Furthermore, incorrect baseline data may have been used, and there were concerns regarding how prognostic factors/effect modifiers were identified, included, and weighted [24]. In the present study, we performed an anchored comparison with the approved dupilumab dose (q2w), reaching qualitatively different conclusions.
In the NMA showing greater efficacy of dupilumab compared with lebrikizumab or tralokinumab for AD (as measured by EASI and POEM) [19], the authors suggested that this difference may be attributed to the known mechanism of action of dupilumab. Unlike lebrikizumab or tralokinumab, which inhibit only IL-13 signaling, dupilumab inhibits both IL-4 and IL-13 signaling, supporting the role of both IL-4 and IL-13 as central and key cytokines involved in the pathogenesis of AD [19]. Noteworthily, pharmacokinetic analyses have demonstrated that the half-lives of both monoclonal antibodies are comparable [25, 26], suggesting that differences in efficacy between dupilumab and lebrikizumab are unlikely to result from variations in their pharmacokinetic profiles.
An additional potential difference between dupilumab and lebrikizumab, which may be related to the role of IL-4 in the pathogenesis of AD, is the onset of action on itch. A change in PP-NRS of ≥ 4 points from baseline was observed for lebrikizumab in ADvocate 1 & 2, where an early significant benefit for lebrikizumab versus placebo was seen at week 2 only in one of these studies (ADvocate 1) [4]. It has been hypothesized that this delay in onset of itch reduction could be reflected by the role of IL-4 in the production of IL-31 [27], although direct comparative evidence is currently lacking. In ADhere, significant improvements for lebrikizumab + TCS versus placebo + TCS were evident from week 4 onward for achievement of EASI-75, ≥ 4-point improvement from baseline in PP-NRS, and ≥ 4-point improvement from baseline in DLQI [3]. In LIBERTY AD CHRONOS, significant improvements for dupilumab + TCS versus placebo + TCS were evident as early as week 2 after the first dupilumab dose for achievement of EASI-75, mean change from baseline in PP-NRS, and ≥ 4-point improvement from baseline in DLQI [28]. Similar rapid improvements in signs, symptoms, and quality of life were observed in the dupilumab monotherapy trials (SOLO 1 & 2) as early as week 2 [29, 30]. However, it is important to note that these observations are based on separate studies and not direct head-to-head comparisons. Further research is needed to confirm any potential differences in the onset of action between these treatments.
Limitations of this study include those innate to ITC comparisons, including a lack of direct evidence (ITCs provide an approximation of relative efficacy) and homogeneity (results may be biased if variations in population demographics or qualities that are treatment effect modifiers are not consistent across trials [17]). However, while ITC analyses may have limited applicability to clinical practice due to differences between study and clinical conditions, this approach provides best evidence where direct head-to-head comparisons are not available.
Looking at the studies included in the analysis of 16-week therapy in combination with TCS, it is evident that more patients included in the ADhere study had IGA 3 at baseline (IGA 3:4 placebo = 73:27; lebrikizumab + TCS = 68:32) versus those in the LIBERTY AD CHRONOS study (IGA 3:4 placebo = 53:47; dupilumab + TCS = 50:50). However, given the other outcomes of interest (EASI, DLQI, PP-NRS) were broadly similar and within standard deviation ranges, this was deemed acceptable for the analyses. The use of concomitant low-to-mid-potency TCS in LIBERTY AD CHRONOS and ADhere was largely similar, although minor differences may have existed.
While this placebo-adjusted Bucher ITC offers important insights into the relative efficacy of dupilumab and lebrikizumab in the absence of direct head-to-head trials, it is important to recognize the inherent limitations of indirect comparisons. Such analyses provide approximations rather than definitive evidence, and prospective comparative studies are needed to conclusively establish real-world effectiveness. Furthermore, although this analysis focuses specifically on dupilumab and lebrikizumab, clinicians must consider the full range of available therapies. Previous NMAs examining multiple treatment options have been discussed in the context of this study, and the current findings should be viewed as one piece of the broader and evolving comparative evidence base.



Comments (0)