
Remember me


A total of 44 patients with AA who were candidates for initiating treatment with baricitinib were included in the study. In total, 66% of the sample consisted of women, with a female:male proportion of approximately 2:1 (29:15). The mean age of the participants was 37.30 ± 16.10 years and 9.10% (4/44) had a family history of AA. Overall, 36% presented some comorbidity of autoimmune origin, with hypothyroidism being the most frequently represented in the sample (20.45%, 9/44).
The mean duration of AA was 10.68 ± 10.24 years. The mean age of debut was 24.80 ± 15.94 years. Among the participants, up to 34.10% (15/44) had total or universal types of AA, and approximately one half (52.27%, 23/44) had involvement of the eyebrows or eyelashes. The most represented type of AA in the sample was multi-plaque (65.90%, 29/44) and the mean SALT index score before starting treatment with baricitinib was 67.16 ± 32.52%.
Regarding previous treatments, all patients had been treated with topical and systemic corticosteroids. Approximately one third of the patients (34.10%) had been treated with classical immunosuppressants and almost one in four (22.73%) had been treated with Tofacitinib with an inadequate clinical response. In terms of TB, the mean score was 2.20 ± 1.29 at baseline. The majority of patients (84.09%) had a low TB, while the remaining participants had a high TB, as they had received at least three cycles of systemic medical therapy prior to starting baricitinib.
Association Between TB and Socio-Demographic, Clinical Factors and Treatment ResponseUnivariate analysis was performed to explore the association between TB and socio-demographic, clinical variables and treatment response (see Table 2). TB was not statistically significantly associated with any sociodemographic variable or with the impact on quality of life attributed to AA (p > 0.10). There was also no association with age at onset, time of evolution, basal SALT or involvement of special locations (p > 0.10). A statistically significant association was observed between TB and SALT score reduction at 6, 9 and 12 months after starting treatment with baricitinib (p < 0.05). This association was maintained after multivariate analysis.
Table 2 Univariate analysis to study the association between therapeutic burden (TB) categorised as low (scores < 3) and high (scores ≥ 3) and rest of variables studied in the sampleImpact of TB on the Real-World Effectiveness of BaricitinibA multivariate analysis using a logistic regression model was performed to control for potential confounding factors. The analysis was adjusted for the main known response factors in patients with AA initiating treatment with baricitinib (disease duration, total or universal forms of AA, baseline SALT score and sex) [9] as well as for TB. A lower TB and shorter disease duration were found to be statistically significantly associated with a greater treatment response (p < 0.05). This association was independent of the other variables studied (see Table 3).
Table 3 Multivariate analysis to study the association between SALT reduction during the first year of treatment and TB, controlling for the main known predictors of response (female sex, duration of AA, severity of AA and total or universal forms of AA)Low TB was statistically significantly associated with a greater reduction in SALT at 6 and 9 months of treatment (p < 0.05) and showed a trend towards statistical significance at 12 months (p = 0.07). Shorter disease duration was statistically significantly associated with a greater reduction in SALT at 3, 6 and 9 months of treatment (p < 0.05). Sex, basal SALT score and total or universal forms of AA were not associated with treatment response (p > 0.10) (see Table 3).
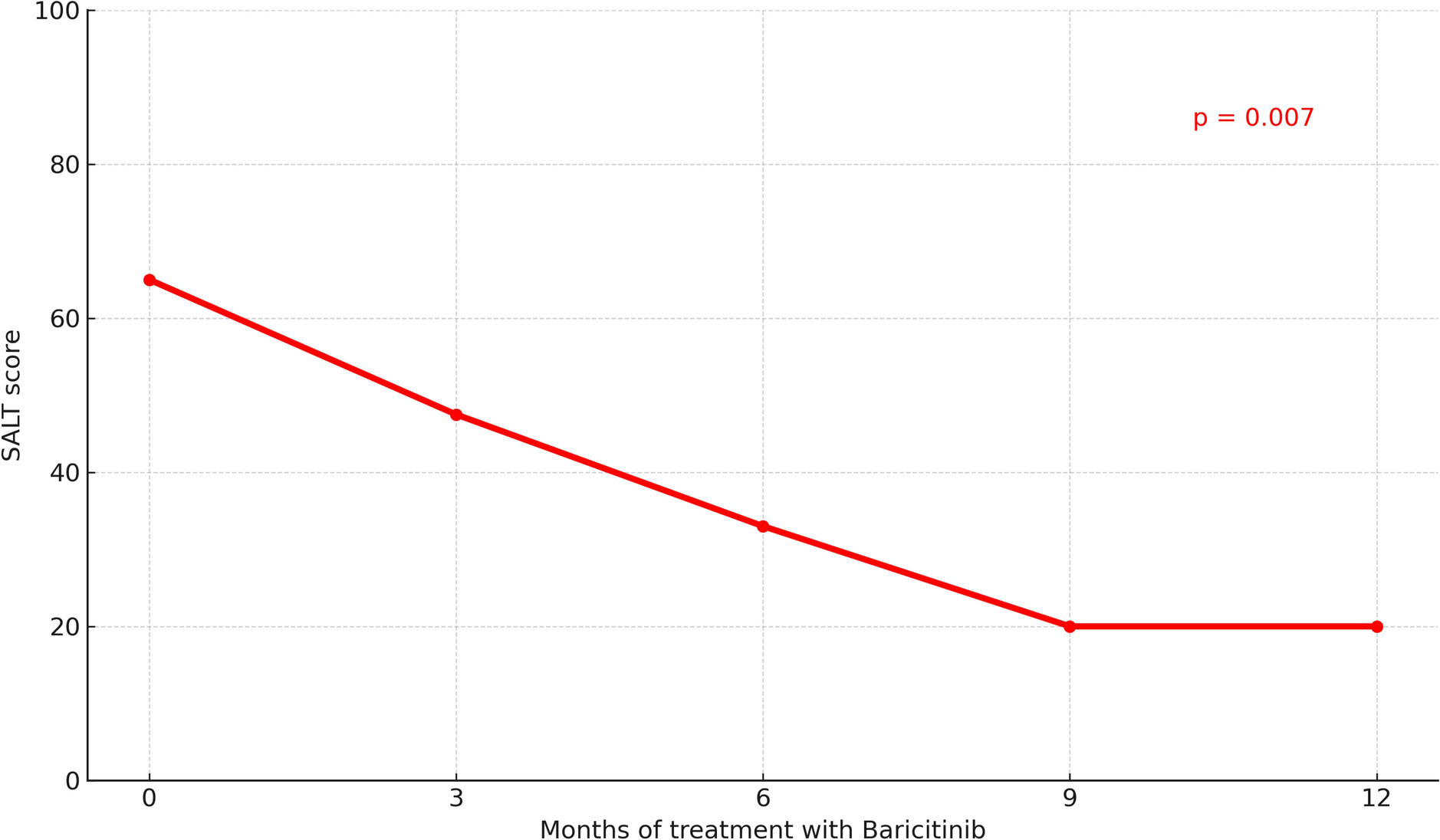
Effectiveness and Safety of Baricitinib for the Treatment of AA in Real-World Clinical PracticeA statistically significant and progressive reduction in median SALT scores (p = 0.007) (see Fig. 1) and in SALT-25, SALT-50 and SALT-75 was observed during quarterly visits after completing 1 year of treatment with baricitinib (see Table S1 in the electronic supplementary material for details).
Fig. 1
Longitudinal evolution in mean Severity of Alopecia Tool (SALT) score over 12 months of baricitinib treatment in patients with Alopecia Areata (AA). A significant decrease in SALT score was observed from baseline score (p = 0.007). Data are shown as mean SALT scores at each time point
Patients with a low TB demonstrated a mean reduction in the baseline SALT score of 53.16% at six months and 69.80% at 12 months, whereas this reduction was 16.10% at 6 months and 30.40% at 12 months for patients presenting a high TB at the initiation of treatment (p = 0.009) (see Fig. 2).
Fig. 2
Evolution of SALT scores over 12 months of baricitinib treatment in patients with AA, stratified by Therapeutic Burden (TB). Patients were categorized into High (≥ 3 previous treatments, red line) and Low (< 3 previous treatments, blue line) TB groups. A consistent reduction in SALT score was observed in both groups, with significantly greater improvement in the Low TB group (p < 0.05). Data are presented as mean SALT scores over time
The drug was shown to be safe for most patients, with a low incidence of adverse effects, among which acneiform reactions (17.60%), elevated cholesterol values (7.80%) and increased transaminase levels (4.55%) were the most remarkable. None of the participants had to discontinue treatment during the study.
Comments (0)