
Remember me


After study eligibility criteria were applied, 475 patients were identified from the registry, consisting of 220 patients with BSA 3–10% and 255 patients with BSA > 10%.
Among patients with BSA 3–10%, 24 discontinued risankizumab and 73 did not have a follow-up visit at 12 months. Among patients with BSA > 10%, 24 discontinued risankizumab and 82 did not have a follow-up visit at 12 months. Thus, analysis included 149 patients with BSA > 10% and 123 patients with BSA 3–10%, of which subgroups of 78 and 105 had any high-impact area involvement and prior topical therapy experience, respectively.
Baseline demographics and disease characteristics are summarized in Table 1. Among patients with BSA 3–10%, the mean (SD) age, PASI, BSA, and DLQI scores were 47.3 (15.4) years, 6.8 (3.7), 6.7% (2.5), and 8.8 (5.9), respectively.
Table 1 Patient demographics and baseline disease characteristicsAmong patients eligible for systemic therapy per IPC classification, the mean (SD) age, PASI, BSA, and DLQI scores were 46.6 (14.6) years, 14.4 (7.1), 25.2% (17.3), and 9.7 (6.1) among patients with BSA > 10%, 47.7 (16.1) years, 6.4 (3.6), 6.5% (2.6), and 9.0 (5.7) among patients with BSA 3–10% with any high-impact area involvement, and 47.4 (15.2) years, 6.8 (3.8), 6.6% (2.6), and 9.2 (5.9) among patients with BSA 3–10% and prior topical therapy experience, respectively.
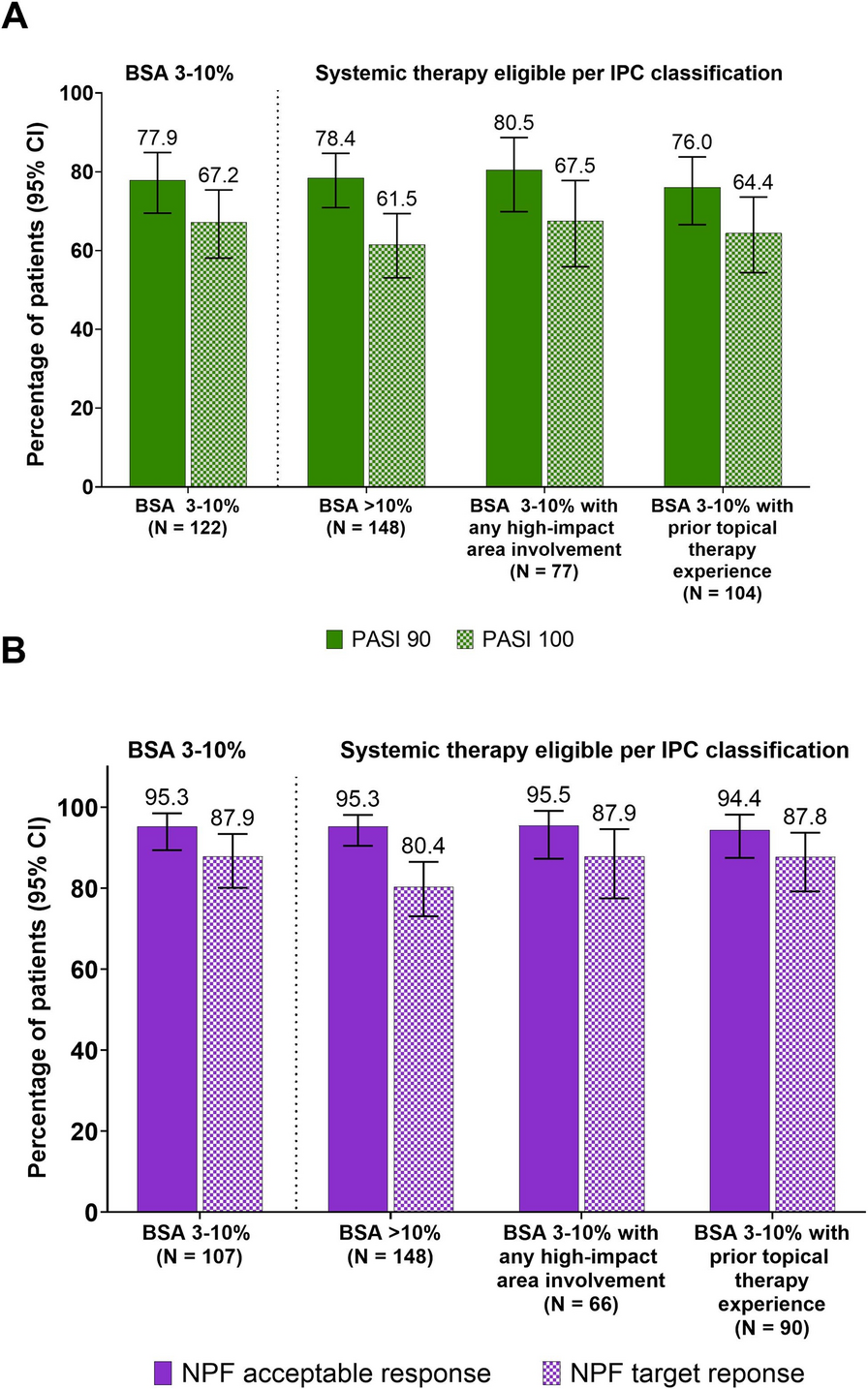
Clinical EffectivenessAchievement of Skin ClearanceAt 12 months, rates of achievement of PASI 90 and PASI 100 were consistent regardless of disease severity classification (Fig. 1a). Among patients with BSA 3–10%, PASI 90 and PASI 100 were achieved by 77.9% and 67.2%, respectively.
Fig. 1
Achievement of skin clearance among patients treated with risankizumab for 12 months by IPC classification of disease severity. a Percentage of patients achieving PASI 90 and 100. b Percentage of patients achieving NPF treatment target goals. BSA body surface area, IPC International Psoriasis Council, NPF National Psoriasis Foundation, PASI Psoriasis Area Severity Index
The percentage achieving PASI 90 and PASI 100 was 78.4% and 61.5% of patients with BSA > 10%, 80.5% and 67.5% of patients with BSA 3–10% with any high-impact area involvement, and 76.0% and 64.4% of patients with BSA 3–10% with prior topical therapy experience, respectively.
Achievement of NPF Treat-to-Target GoalsAt 12 months, most patients achieved NPF treatment target goals irrespective of disease severity classification (Fig. 1b). Among patients with BSA 3–10%, NPF acceptable and target responses were achieved by 95.3% and 87.9%, respectively.
The NPF acceptable and target responses were achieved by 95.3% and 80.4% of patients with BSA > 10%, 95.5% and 87.9% of patients with BSA 3–10% with any high-impact area involvement, and 94.4% and 87.8% of patients with BSA 3–10% and prior topical therapy experience, respectively. All groups achieved significant improvements in PASI and BSA 12 months from baseline (P < .001, Fig. 2).
Fig. 2
Mean percent improvement in PASI and BSA among patients treated with risankizumab for 12 months. BSA body surface area, IPC International Psoriasis Council, PASI Psoriasis Area Severity Index
Achievement of PROsDLQIRegardless of disease severity classification, most patients achieved DLQI 0/1 (Fig. 3). Among patients with BSA 3–10%, DLQI 0/1 was achieved by 68.1%.
Fig. 3
Achievement of DLQI 0/1 among patients treated with risankizumab for 12 months by IPC classification of disease severity. BSA body surface area, DLQI Dermatology Quality of Life Index, IPC International Psoriasis Council
Among patients with BSA > 10%, BSA 3–10% with any high-impact area involvement, and BSA 3–10% with prior therapy topical experience, DLQI 0/1 was achieved by 76.3%, 66.7%, and 64.9%, respectively.
Among patients with BSA 3–10%, the mean (SD) improvement in DLQI from baseline was 7.4 (5.7) (P < .001). Among patients with BSA > 10%, BSA 3–10% with any high-impact area involvement, and BSA 3–10% with prior topical therapy experience, the mean (SD) improvement in DLQI was 8.1 (6.4), 7.6 (5.8), and 7.6 (5.8), respectively (P < .001, Table 2).
Table 2 Change in health-related quality of life from baseline to 12 monthsSkin Pain, Overall Itch, and FatigueAll groups of patients reported significant reductions in skin pain, overall itch, and fatigue from baseline (Table 2). Among patients with BSA 3–10%, the mean (SD) improvements in skin pain, overall itch, and fatigue scores were 25.1 (31.9), 43.7 (31.5), and 17.6 (32.4), respectively (P < .001).
The mean (SD) improvements in skin pain, overall itch, and fatigue scores were 34.0 (31.7), 50.3 (36.6), and 16.9 (32.5) among patients with BSA > 10%, 26.1 (33.4), 45.5 (32.1), and 19.5 (31.4) among patients with BSA 3–10% with any high-impact area involvement, and 25.5 (31.2), 43.5 (31.5), and 15.9 (32.5) among patients with BSA 3–10% and prior topical therapy experience, respectively (P < .001).
Work and Activity ImpairmentAll groups of patients reported significant improvements in work and activity impairment. Among patients with BSA 3–10%, the mean (SD) improvement in work and activity impairment was 11.3 (16.6) and 16.4 (25.4), respectively (P < .001).
The mean (SD) improvement in work and activity impairment was 13.7 (27.0) and 23.8 (30.7) among patients with BSA > 10%, 11.2 (14.4) and 17.7 (26.2) among patients with BSA 3–10% with any high-impact area involvement, and 10.4 (15.5) and 15.3 (24.9) among patients with BSA 3–10% and prior topical therapy experience, respectively (P < .001).
Comments (0)