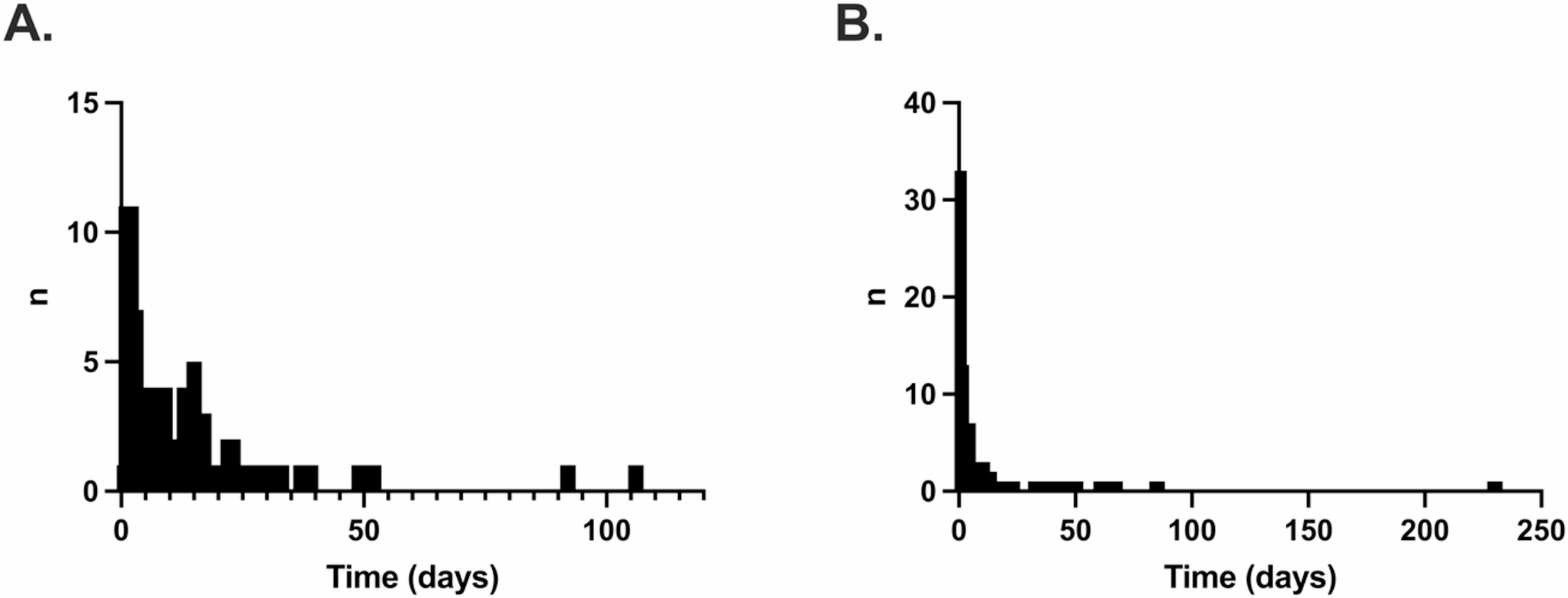
In this first study on ACSC rehospitalizations after sepsis in Germany, we found that one third of sepsis survivors is affected by ACSC rehospitalizations in the 12-months post-discharge. ACSC rehospitalizations often occur closely after discharge and more frequently affect older, male, care dependent patients as well as those living in rural areas. 21.3% of ACSC are infection-related and therefore may be partially vaccine-preventable, which can offer important targets for preventive measures to reduce the burden of sepsis.
Our ACSC rehospitalization rates are comparable with the proportion of ACSC rehospitalizations in sepsis found in a US study among veterans aged 65 years and above (37% in our study vs. 42% in the US), but higher than among general ICU survivors in the US (24% of rehospitalizations) [13]. The ACSC proportion among hospitalizations is also higher than estimated in the general German population (27% in 2012), which may underline the vulnerability of sepsis survivors in terms of recurrent infection and sepsis, but also cardiovascular and pulmonal diseases of which many are considered ambulatory-care sensitive.
In our studies, risk groups for ACSC rehospitalizations comprised older, male, care dependent patients and those living in rural communities. Intestingly, the odds for ACSC rehospitalization were lower in nursing home residents than in care dependent patients living in the community compared to a reference of non-care dependent patients. We hypothesize that this may be due to the fact that in Germany, each nursing home is typically affiliated with a designated general practitioner (GP) who is responsible for providing primary medical care to the residents. While residents formally retain the right to choose their own physician, in practice, many receive care from the nursing home’s assigned GP to ensure continuity and better coordination of care. This model facilitates close collaboration between medical staff and nursing personnel and supports timely medical interventions within the facility, which may contribute to a better prevention of ACSC rehospitalizations compared to patients with nursing care degree receiving care outside nursing homes. In this regard, a nationwide German study observed that nursing-home residents had significantly more contacts with general practitioners, medical specialists, and prescriptions for medical aids than their home-dwelling counterparts [14]. In rural patients, the higher ACSC risk may be driven by limited access to primary care and specialist services, longer travel distances to healthcare facilities and limited availability of public transportation [15], and an increasing shortage of healthcare professionals in these regions [16].
The high ACSC rehospitalization rates we observed, particularly closely after discharge, underscore the importance of seamless follow-up care in sepsis survivors, with a focus on physical rehabilitation, structured (outpatient) aftercare and social support measures for patients and their families [17, 18], and tailored to align with both the available resources and the living environments risk groups. To this end, a transitional care intervention with focus on care coordination, including screening on sepsis sequelae, management of chronic diseases and advance care planning was effective in reducing a composite endpoint of rehospitalization and mortality in sepsis survivors in a recent US randomized control trial [19]. Furthermore, immunization gaps should be closed and thereby can contribute to the prevention of infection-related ACSC, but also cardiovascular sequelae [20]. However, it also has to be acknowledged that only a certain proportion of ACSC rehospitalizations may be preventable by improved (ambulantory) aftercare. Therefore, the impact of aftercare interventions on ACSC rehospitalization rates and their preventability needs also be evaluated in further studies.
Limitations
We used health claims data that are collected for reimbursement purposes and therefore may be influenced by external incentives within the DRG system. In this data, sepsis may be identified only with low sensitivity, and cases with lower severity may be missed [21]. This may similarly apply for ACSC, although we lack data on the validity of coding for these conditions in Germany. Second, our data did not include patients without sepsis, thus we cannot make any conclusions if ACSC occur with higher frequency compared to other acute medical conditions. Third, we cannot trace individual patient paths to understand which diagnostics and treatments patients with ACSC received prior to their hospitalization in the outpatient setting, as outpatient diagnoses are only available on quarterly basis in Germany.



Comments (0)