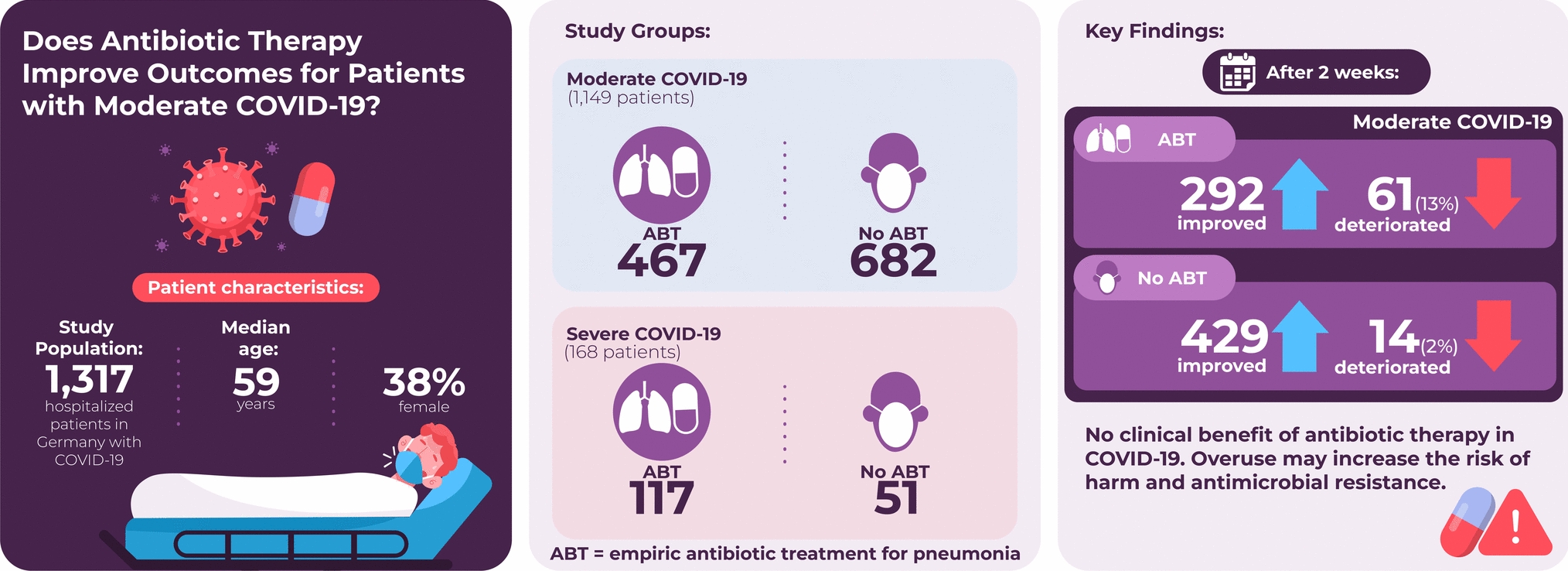
In this study, we address this critical question using the largest German cohort available through the German National Pandemic Cohort Network (NAPKON) [8]. Patients were grouped based on whether they received ABT upon hospital admission or not. Primary outcome of our study was improvement or decline in health after two weeks as measured by change in WHO score.
WHO clinical progression scale
The WHO score was used in this study to assess patient severity (Online Resource Supplementary Table S1) [7].
Study objectivesPrimary objective
The primary objective of the study was to compare clinical outcomes between patients who did and did not receive antibiotic treatment (ABT) at baseline (i.e., at study enrollment). The study population consisted of patients with moderate COVID-19 at baseline (WHO score 4, 5). The primary outcome was improvement or decline in health defined by an increasing or decreasing change in WHO score between baseline visit and two weeks later.
Secondary objectives
The secondary objectives were the following:
Compare patients with moderate COVID-19 at baseline with and without ABT with respect to the outcomes health decline (decreased WHO score) and death during the observation period (hospital stay and follow-up).
The same as for primary and first secondary objectives but for the population of patients with severe COVID-19 disease at baseline visit (WHO score 6–9).
Study cohort
The National Pandemic Cohort Network (NAPKON, https://napkon.de/projekt-napkon), established a comprehensive cross-sectoral COVID-19 cohort in Germany (SUEP), tracking patients from infection onset up to three years. The study employs standardised procedures and biosample storage. This cohort represents a national, multicenter, minimally interventional prospective cohort study of patients diagnosed with SARS-CoV-2 infection, including procedures such as taking blood cultures and swabs, collection of urine and respiratory samples and surveys. The study design allowed for patients to receive a baseline visit and defined follow up visits (weekly, if clinical deterioration, end of acute phase, discharge, death if applicable, telephone follow-ups every six weeks post-infection, at three and 12 months). All patients gave written informed consent prior to their inclusion.
Our study was approved by the Ethics Committee of the Medical Faculty of the University Hospital Schleswig–Holstein, Kiel, Germany (Approval Number: D595/21).
Inclusion and exclusion criteria
We considered visit data from March 2020 to May 2023. Inclusion in the study required a positive SARS-CoV-2 PCR test at hospital admission, at least a baseline and a discharge visit, being hospitalized, at least 18 years old, and available information on ABT seven days prior to baseline to four days after baseline. Patients had to be classified according to moderate (WHO score 4, 5) or severe (WHO score 6–9) COVID-19. Patients with directed ABT due to foci other than the lung (e.g. with pathogenic organisms in stool or ascites) were excluded. Furthermore, patients on palliative care were excluded due to other aims of therapy. Quality checks of data identified one patient with an implausible baseline date who was excluded from the study.
Antibiotics and microbial diagnostics
In our study, we focused solely on antibiotics commonly used in the treatment of respiratory infections. The antibiotics included were acylureidopenicillines combined with a β-lactamase inhibitor (BLI), aminopenicillines with or without BLI, carbapenemes, second to third generation cephalosporines (including subgroup 3b), fluoroquinolones, macrolides, and tetracyclines (Online Resource Supplementary Table S2). With regard to relevant pathogens, we took into account microbiological results from seven days before and four days after the baseline visit. Three infectious disease specialists defined relevant diagnostic materials and independently rated whether pathogens were the likely origin of pneumonia and required appropriate ABT. Differences were resolved through discussion.
Statistical analyses
Assuming a 20% proportion of health decline in the study population of patients with moderate COVID-19 who experienced a change in health status within two weeks, a sample size of at least 219 patients in both the ABT and non-ABT groups is required to detect a 10% difference in the proportion of health decline. This calculation is based on a significance level of 0.05 and a statistical power of 0.80, using a Chi-squared test with Yates correction (BIAS for Windows, Version 11.12).
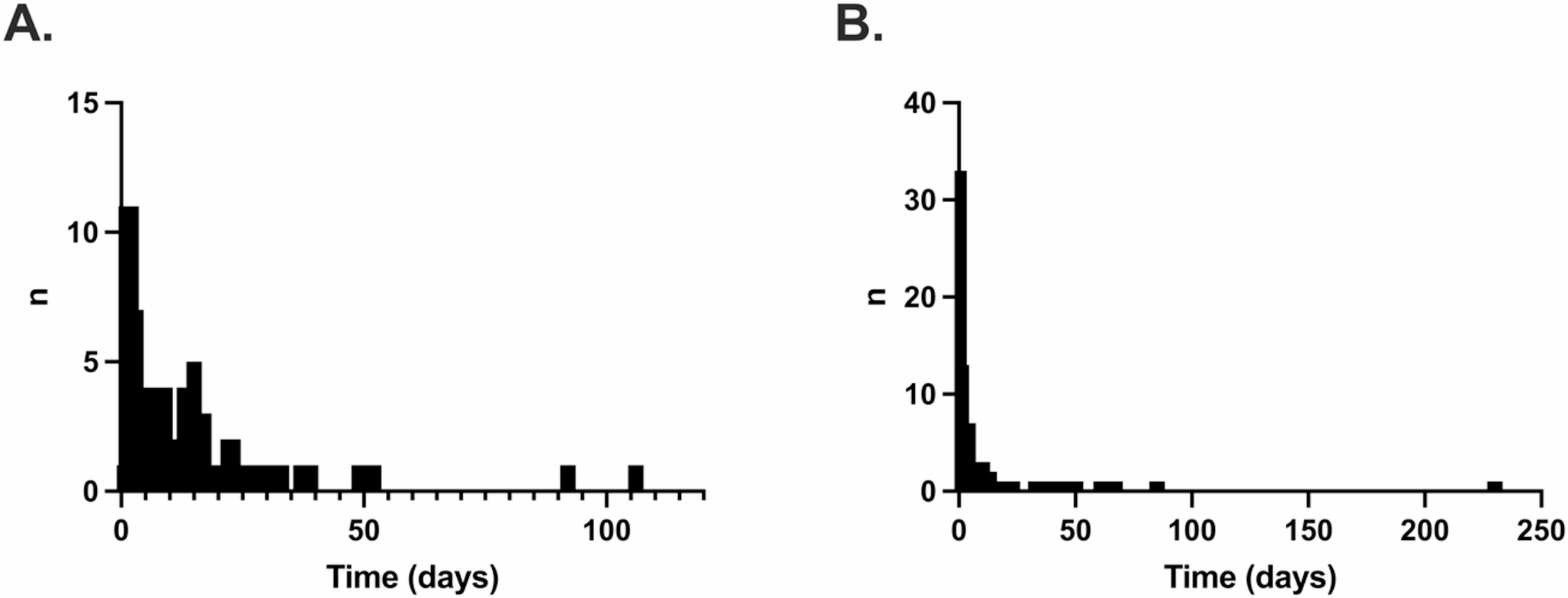
The WHO score was calculated for each patient at every documented visit. We defined deterioration or improvement by comparing the WHO score at baseline with a later visit. For the primary outcome, time interval was set at 14 days after baseline. If no visit occurred exactly 14 days post-baseline, the visit closest prior to 14 days post-baseline was included in the analysis. Since additional visits were conducted if the patient’s health deteriorated, the visit closest to the 14-day mark is likely to reflect the patient’s health status at that time. For any discharge or death occurring within the 14-day period the WHO score was adjusted accordingly.
All variables were categorised in groups. Descriptive statistics show absolute and relative percentages. For univariable analyses with ABT or clinical improvement/decline as outcome we applied Fisher’s exact test. Multiple logistic regression with ABT status (yes/no) as outcome was performed to identify factors relevant to ABT prescription. Furthermore, multiple logistic regression analysis was used with improvement/decline after two weeks (primary outcome) and health decline and death during hospital stay (secondary outcomes) to investigate the influence of ABT adjusted for additional covariables and potential confounders.
In both cases, we chose clinically relevant factors as influence variables. These had to be sufficiently documented with a sufficient frequency of recorded events. We therefore summarized single comorbidities in the updated Charlson Comorbity Index CCI. No interactions were considered and no imputation for missing values was used. For the logistic model, we applied backward selection with a significance threshold of 0.05. Results of multiple regression analyses are presented as odds ratios with 95% confidence intervals. Additionally, Nagelkerke’s R2 was calculated as a measure of goodness of fit. The outcome death was additionally analysed by the Kaplan–Meier method and groups with and without ABT were compared with a log rank test. No Cox regression was performed because the proportional hazard assumption was strongly violated.
To test the robustness of our results and especially to account for differences in risk factors like comorbidities between patients receiving ABT and those who did not, a propensity score analysis with matching was conducted. For this, the R package MatchIt was utilized [9]. The propensity score was calculated using a logistic regression model and all covariables significant in the univariable analysis (Table 2; age, gender, documented pathogen detection, vaccination, frailty, CCI). For matching, a ratio of 1:1 with respect to patients with and without ABT was applied and we utilized the nearest neighbor approach and a caliper of 0.1. The matched dataset included 426 patients (213 with and 213 without ABT). After matching, the groups of patients with and without ABT showed good balance with respect to the selected covariables (Online Resource Supplementary Table S3). The primary outcome improvement vs. decline in health after two weeks was then compared between patients with and without ABT on the matched data by first performing a logistic regression with improvement/decline as outcome and ABT and covariables as influence variables, utilizing the weights of the propensity score matching and applying the argument ‘family = quasibinomial’ for more robustness. After that group comparison was performed with the function avg_comparison of the R package marginaleffects [10] to derive odds ratios and the 95% confidence interval using the subclasses of the propensity matching for the argument ‘vcov’. This accounts for matched individuals by a cluster-robust method. We repeated the analysis excluding patients with documented pathogens.
All analyses used a two-sided significance level of p = 0.05 and were performed with the statistics software R, Version 2023.06.1 + 524 [11].



Comments (0)