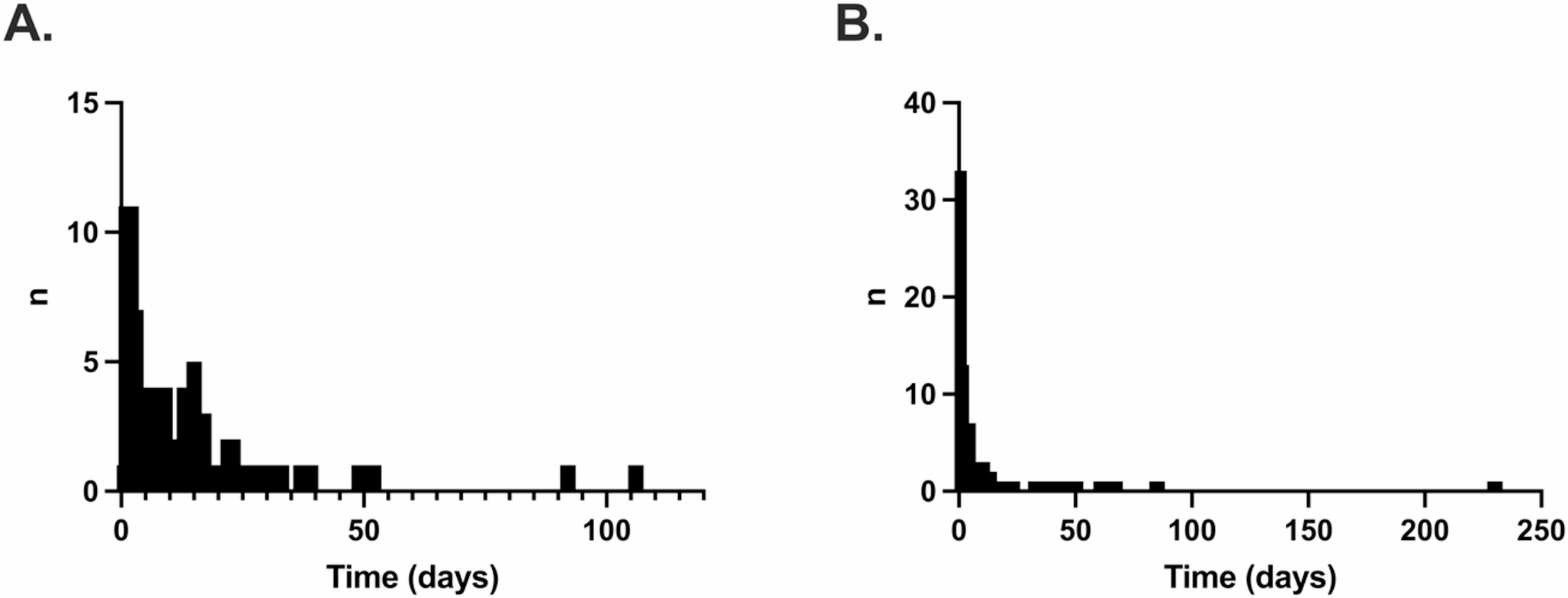
In this analysis of transitional care in sepsis patients, we found that sepsis survivors had a high frequent, multisector health care utilization in the 90 days post-sepsis. More than one third of survivors had at least one emergency treatment during that period. As common first health care provider contact, the GP plays a particular role in Germany, especially in patients of higher age, with chronic care needs and those who were treated outside the ICU setting. Of note, first health service provider contacts occurred with low latency of 0–7 days post-sepsis in median and nearly all patients had health care contacts in the quarter post-sepsis. This latency and the proportion of patients who died without further health care contacts post-sepsis, however, was considerably elevated during the first wave of the Covid-19 pandemic.
Our results are in line with previous research that confirms frequent post-acute readmissions in sepsis survivors [9]. According to a recent meta-analysis, 90-day readmission rate was 38.1% in sepsis survivors [9] and higher than in any other acute diseases [16], which may reflect a prolonged recovery period due to the severity of the acute disease, as well as chronic long-term impairments which can arise from lasting alterations in immune function and organ damage caused by the acute sepsis [17, 18]. In a matched US-cohort study, 42.6% of sepsis survivors were hospitalized in the 90 days post-sepsis, with a higher proportion of outpatient-care sensitive conditions (ACSC) than in patients with other acute medical diagnosis (42% vs. 37% of all readmissions) [16]. These ACSC hospitalizations are considered potentially preventable hospitalizations by early outpatient care [19], which underlines the opportunity to prevent hospital readmissions by seamless hospital follow-up for this vulnerable patient group.
To this end, our data confirm that nearly all survivors had early health care contacts in the 90 days post-discharge. More than two thirds of sepsis survivors were first treated by their GP, and more than 80% were first treated by a GP or other outpatient physician after their hospitalization, which therefore can be considered important stakeholders in transitional sepsis care with the potential to facilitate screening and coordinate treatment of post-sepsis sequelae. Nevertheless, in Germany, the structure of post-sepsis care remains highly heterogeneous, with no unified national guidelines or standardized care pathways, leading to considerable variability in follow-up practices and access to support services. Patients still subjectively report a lack of follow-up care, particularly with regard to coordination and sepsis-specific orientation in Germany [20]. This may be due to hurdles that currently hinder the provision of aftercare tailored to the needs of sepsis survivors in this context, including the lack of guidelines for specific aftercare after sepsis [11], the suboptimal information sharing between ICU and GPs, and capacity strains, e.g. in the availability of outpatient physical therapy [21]. Furthermore, GPs describe a scarcity of experience and knowledge on the aftercare of sequelae after critical illness due to their low incidence in the primary care context [21, 22], which underpins the potential of education on post-acute sepsis care for health care providers as a prerequisite for an improved aftercare [11]. The transition may also be facilitated by structured programs initiated during the acute hospitalization. In this regard, a recent randomized-controlled trial found that a nurse navigator program which started during the hospital stay and continued after discharge to initiate a review of the patients’ medication, the evaluation for new impairments or symptoms, the monitoring comorbidities, and palliative care approach when appropriate was effective in reducing a combined endpoint of 30-day readmissions and mortality [8].
Our study also marks differences in the provision of transitional care pre- and during the COVID-19 pandemic. Notably, the proportion of patients without post-sepsis health care contacts was elevated, the frequency of post-acute rehabilitation decreased, and the latency of first health service provider contacts increased in 2020 compared to 2016–2019. Similar observations were made for other acute and post-acute diseases in Germany, e.g. with longer durations between symptom onset and hospital treatment for acute cardiovascular diseases [23] or a lower number of rehabilitation treatments after stroke [24]. In the future, it seems therefore important to develop ways to keep the routine care of patients with acute illnesses requiring urgent care stable to prevent avoidable deaths and other adverse outcomes in the event of further public health crises.
This study has several strengths, including the comprehensive, population-based database with reliable data on health service provider contacts including more than 27 million insurance holders of the AOK in Germany. Precise operationalizations were developed to record health care utilization and outpatient contacts as comprehensively as possible. In particular, the operationalizations of physician-patient contacts via fee schedule positions and treatments in emergency departments provide novel insights compared to previous works. Another strength is that the study is that it is not subject to selection and healthy volunteer bias, as data from all AOK-beneficiaries could be included. This form of bias is often relevant in patients receiving life-threatening or intensive medical care, as their ability to give consent may be impaired.
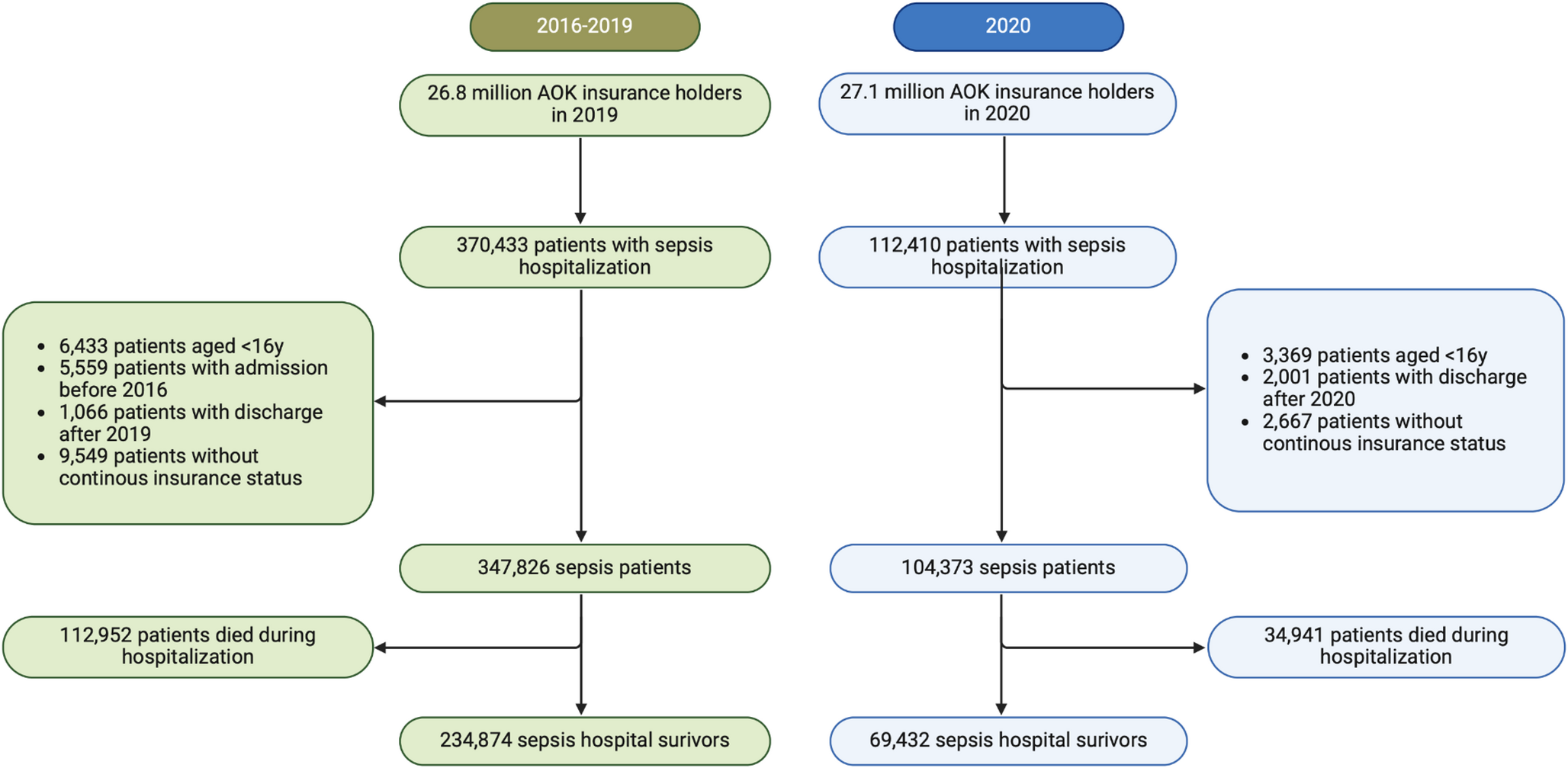
However, there are also limitations to consider. We used nationwide health claims which were originally generated and collected for billing purposes. Previous validation studies showed an underestimation of sepsis cases in these data, as not all cases are diagnosed and coded as such, particularly if the sepsis severity is low [25]. Due to the billing processes in the outpatient sector, which occur on a quarterly basis, outpatient physician-patient contacts are likely underestimated because not all treatments can be billed separately, partly depending on the patient’s morbidity. This must be taken into account when interpreting the results. Furthermore, we cannot draw any conclusions about individual patient pathways and treatment decisions. We do not expect substantial differences in post-acute sepsis care between individuals insured by the AOK and those covered by other statutory health insurance providers in Germany, as the overall structure and access to services within the statutory health insurance system are largely comparable across health insurance providers. However, we cannot rule out demographic or socioeconomic differences between AOK-insured and non-AOK-insured populations [26], which may limit the generalizability of our findings to some extent. Moreover, it has to be noted that the 2016–2019 and 2020 cohorts are not directly comparable due to changes in coding guidelines in Germany and the incorporation of COVID-19 related sepsis cases in the 2020 cohort.



Comments (0)