
Remember me

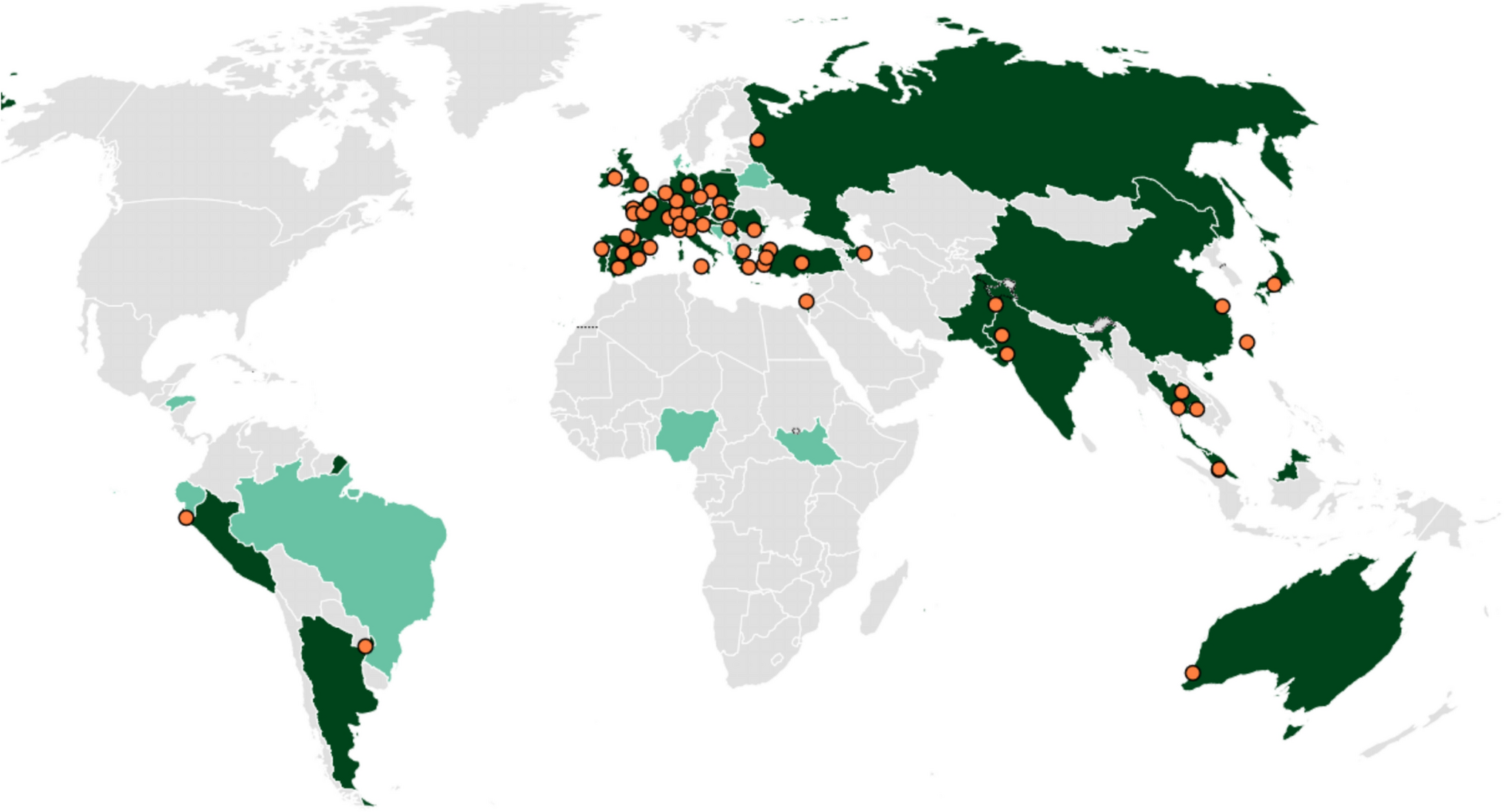

This study utilized a descriptive, cross-sectional design. An initial invitation to participate in the study was distributed through the Infectious Diseases International Research Initiative (ID-IRI) network, a voluntary academic community of ID specialists and trainers. A detailed information letter accompanied the invitation, clearly outlining the aim, scope, and voluntary nature of the study. The letter emphasized that the survey sought structured, national-level data on ID specialty training, not personal opinions or institutional data, and that participation was anonymous and voluntary. Respondents, were instructed to complete the questionnaire independently and encouraged to consult national guidelines or authorities if needed. A total of 29 scholars from 29 different countries, qualified professionals actively involved in ID specialty training programs, participated in the study and provided national-level insights. Although only one respondent per country was included, which may limit generalizability within each country, this approach ensured consistency and allowed for systematic cross-country comparison of training structures and policies. The participants represented five geographic regions: Central Asia (Azerbaijan, Uzbekistan, Kyrgyz Republic, and Kazakhstan), the Middle East (Iran, Saudi Arabia, Jordan, Iraq, Oman, United Arab Emirates, Qatar, and Lebanon), the Southeast Europe (Albania, Greece, Kosovo, Slovenia, Bosnia and Herzegovina, Serbia, Republic of North Macedonia, and Croatia), Eastern Europe (Russia, Moldova, Romania, and Bulgaria), South Asia (India and Pakistan, Afghanistan), Southeast Asia (Malaysia), and Türkiye (Fig. 1).
Fig. 1
Countries included in the study are marked in dark grey color [Generated using MapChart.net]
This study did not involve patients, medical records, clinical interventions, or any sensitive personal data. It surveyed ID specialists or trainers about the structure and policies of postgraduate ID training in their respective countries. All information provided by participants was based on publicly known or professionally accessible training structures, and no institutional or confidential data were used. The data collection tool was developed specifically for this study. Participation was fully voluntary and anonymous, and no incentives were offered. Informed consent was implied through participants' voluntary completion of the online questionnaire.
Data collection and analysisA structured data collection tool (Supplement 1) was developed by a professional team comprising one medical education specialist and three ID specialists. The tool was informed by relevant references and existing literature to ensure content validity and comprehensiveness. It was pilot-tested with three independent ID specialists and reviewed by two medical education experts. Feedback from this process was incorporated to enhance clarity and usability. The final questionnaire consisted of three main sections:
Part 1 – Professional Background: Focused on general professional information, such as academic title, country of practice, and primary specialty. No personally identifiable or sensitive data were collected.
Part 2 – General Structure of ID Practice and Training: Explored the national structure and current status of ID specialty training, using 19 targeted questions (both multiple choice and open-ended) designed to assess the scope, organization, and challenges of ID practice in each country.
Part 3 – ID Specialty Training Curriculum: Assessed the specific components of ID specialty curricula through 10 multiple choice and open-ended questions, addressing duration, comprehensiveness, and educational content.
A total of 29 participants from 29 countries completed the questionnaire independently via Google Forms between 15 October and 30 November 2024. Two reminder emails were sent during the data collection period to encourage full participation. In cases of incomplete or unclear responses, participants were encouraged to consult relevant authorities or provide explanatory comments. Although only one qualified respondent per country contributed, limiting generalizability within each nation, this approach ensured consistency and enabled systematic cross-country comparison.
Descriptive statistics were used to summarize all survey responses. To explore regional differences in categorical variables, whether ID is recognized as an independent specialty or whether a thesis is required, Fisher’s exact test was applied due to small expected frequencies in some cells. For continuous variables, such as training duration, number of training centers, and number of trainees, one-way ANOVA was used to assess variation across regions, based on the United Nations regional classifications. A p-value of < 0.05 was considered statistically significant.
ResultsThe study included participants from 29 countries, representing a diverse range of medical professionals specializing in ID and related fields. Of the participants, 20 specialized in infectious diseases, 2 in both infectious diseases and Clinical Microbiology, 2 in Clinical Microbiology, 4 in both infectious diseases and internal medicine and 1 in infectious diseases and Pediatrics. The participants represented a variety of academic titles, such as MDs, MScs, PhDs, Assistant Professors, Associate Professors and Full Professors.
Variations in ID specialty configuration across different countriesParticipants from nineteen (65.5%) countries indicated that ID is recognized as an independent specialty program that can be pursued directly after medical school in their country. In countries such as Greece, Jordan, Oman, Qatar, Pakistan, India, Lebanon and Malaysia, ID is pursued as a specialty following the completion of Internal Medicine. In the United Arab Emirates and Saudi Arabia, ID is a specialty pursued after completing internal medicine or pediatrics (Table 1). No statistically significant association was found between geographic region and the organization of ID as an independent specialty (Fisher’s exact test, p = 0.545).
Table 1 General structure of ID specialty training programsPathways to ID specialtyParticipants from seventeen (59%) countries reported a required exam for entry into the ID specialization, administered by national authorities (n = 13) or local authorities (n = 4). A written exam was not required in 11 (34%) countries, in Oman written exam requirement was reported for IM specialization prior to ID. The names of the entrance exams for each country are listed in Table 1. In Russia, the exam is conducted by national authorities as a primary accreditation after graduation from medical school (with scores), which serves as the admission examination for residency in ID and other specialties (Table 1).
Occupancy rates for ID training positionsParticipants were asked to indicate the occupancy rate (%) of the available training positions for ID in the most recent specialty exams in their country. Professionals from Greece, Azerbaijan, Oman, Qatar, Romania, Iraq, Moldova, Afghanistan and Uzbekistan reported a 100% occupancy rate for available ID training positions in the most recent specialty exams in their countries. Russia similarly reported 95–100% occupancy rate. Croatia and the Kyrgyz Republic reported a 90% occupancy rate, while 15 other countries reported an occupancy rate over 80%. Five professionals were unable to provide any data (Table 1).
Perception of ID specialty in a post-COVID eraThe general expression of ID specialty in the country following the COVID pandemic was rated on a scale of 1 to 5 (1 = no perceived increase in importance, 3 = moderate change, 5 = clearly perceived increase in importance), with scores ranging from 2 to 5 (mean 3.5). The lowest rating was reported in Slovenia (1), while the highest ratings were in Iraq, Malaysia, and Uzbekistan (5).
Variations in ID specialists and training centers across the countriesThe number of reported ID specialists and training centers varied significantly among the countries. The number of ID specialists ranged from 10 to 7230. Jordan did not report any training centers. While countries such as Kosovo and Albania reported only one and the UAE reported two training centers, Türkiye reported over 80; and Russia reported 81 training centers (Table 1).
Length of ID specialty trainingThe duration of ID specialty training varied, with an average of 4 years (range 1–6 years). Seven countries reported a training duration of 1–2 years, 13 countries had duration with in the 3–4 years range, and seven countries reported duration of 5 or more years. The longest duration, 6 years, was reported from Slovenia (Table 1). A one-way ANOVA showed a statistically significant difference in ID training durations across regions (F (5,23) = 9.40, p < 0.001).
Compulsory training in other institutionsCompulsory period of training in other local centers or abroad included in the ID specialty training program was positive in Kosovo, Oman, Croatia, Saudi Arabia and Kazakhstan. In Kosovo trainees are offered free training periods conducted in other institutions or abroad for ID specialty training curriculum or financed by the individuals themselves. In Oman, ID specialty trainees need to complete a fellowship abroad for at least 2 years. In Croatia, part of the rotations should be performed only at university hospitals (4 regional, including one national university center) in addition to rotations performed in general hospitals, depending on the authorization to conduct specialist training held by an individual health institution, depending on meeting general and special conditions (organization, equipment, number of specific examinations and procedures, number of patients, number of university staff, etc.) prescribed by the rulebook and regulations for each specialization issued by the Ministry of Health. In Saudi Arabia, trainees rotate through various hospitals and may spend one year in Canada, depending on their specialization location and in Kazakhstan a preferred academic program was reported, not mandatory (Table 1).
License renewalIn the study, nine countries reported to have mandatory periodic license exam for ID. The most common renewal period of the exam was every 5 years, in six countries: Azerbaijan, Iran, Russia, Kazakhstan, Kyrgyz Republic, and Moldova. A few exceptions had longer renewal periods, as Croatia (6 years), Serbia and North Macedonia (7 years) (Table 1).
Postgraduate academic career pathwaysIn the majority of the countries (n = 19; 66%) ID specialists may continue their academic career after graduation without obtaining a PhD. However, in some countries (n = 10; 34%) a PhD was mandatory for academic progression. The countries requiring a PhD for academic advancement were Jordan, Azerbaijan, Kosovo, Qatar, Romania, India, Iran, North Macedonia and Malaysia (Table 1).
ID training curriculumNearly all of the countries (n = 27; 93%) reported having a formal ID specialty training curriculum, with the exception of Oman and Serbia. Twenty-four countries (83%) reported having national ID associations in the participating countries. The names and web sites of these associations are listed in Supplement 2.
ID subspecialtiesTen (35%) countries (Bosnia and Herzegovina, Croatia, Iran, Kyrgyz Republic, Oman, Qatar, Russia, Serbia, Türkiye and Uzbekistan) reported that they have some subspecialties under the ID specialty: Intensive Care (n = 6, 21%), Parasitology (n = 4, 14%), HIV&AIDS (n = 4, 14%), Immunology & Allergy (n = 4, 14%), Epidemiology (n = 4, 14%), Microbiology (n = 3, 10%), Hepatology (n = 3, 10%) and Virology (n = 2, 7%). In Türkiye, Immunology & Allergy is replaced with Basic Immunology (Table 2).
Table 2 Subspecialties of ID training programsCurriculum topicsThe curriculum topics related to rational antibiotic use; healthcare-associated infections and critical care/intensive care, and travel medicine were among the most prevalent across the countries. The specialized topic of health economics appeared to be included only in Jordan, while palliative care was included only in Slovenia (Table 3).
Table 3 Distribution of topics in the curriculumInvasive procedural competenciesInvasive procedures that the ID trainees are required to be proficient were listed as; lumbar puncture (n = 23, 79%), urinary catheter insertion (n = 16, 55%), pleural fluid drainage (n = 12, 41%), abscess drainage (n = 6, 21%), endoscopic intervention (n = 3, 10%), bone marrow aspiration (n = 2, 7%), bone marrow biopsy (n = 1, 3%), joint aspiration (n = 1, 3%), central venous access (n = 1, 3%), skin biopsies (n = 1, 3%), endotracheal intubation (n = 1, 3%) and abdominal paracentesis (n = 1, 3%) (for trainees working in the Intensive Care Unit).
Mandatory rotationsThe ID specialty training programs across countries encompass a variety of integral components and mandatory rotations. Internal medicine and microbiology were reported as core components of all programs, followed by infection control, epidemiology, and antimicrobial stewardship (AMS) as essential rotations. Sexually transmitted diseases, travel medicine, and transplantation were included in selected programs. Rotations in Pediatrics, Radiology, Neurology, Hepatology, and Intensive Care were integrated into some curricula. The duration of rotations varies significantly, ranging from 2 weeks to 4 years (Table 4).
Table 4 Integral parts/rotations of ID Specialty Training ProgramEducational methodsAlthough traditional methods such as lectures, didactic sessions, practical exercises, printed materials, manuals, and hands-on workshops were adopted by all countries, educational methods were reported to vary across them. Technology-enhanced methods, including webinars, virtual conferences, and the use of printed materials/manuals, were frequently utilized. Mobile apps, role-playing and scenario-based training were the least adopted methods, appearing only in a few countries, such as Croatia, Russia, Türkiye and Kazakhstan (Table 5).
Table 5 Educational methods in ID training programsAssessment methodsAssessments of ID trainees are listed in Table 6. The logbook/portfolio (n = 19; 66%) was the most commonly used assessment method, followed by the annual progress/professional development exam (n = 16; 55%). The most frequently reported summative formal exams were written exams (n = 17; 59%), oral exams (n = 14; 48%), and clinical exams (n = 13; 45%). The objective structured clinical examination (OSCE) was the least frequently used method, appearing in only 2 countries. The thesis requirement, referring to the mandatory submission of a research-based or project-based document as part of the criteria for completing ID specialty training, was mandated by only 7 countries (24%) in the dataset (Table 6).
Table 6 Assessment of ID traineesFisher’s exact test was used to examine associations between categorical variables such as specialty independence (p = 0.545), thesis requirement (p = 1.000), and OSCE implementation (p = 1.000) across selected geographic regions. No statistically significant associations were observed.
Comments (0)