
Remember me


In March 2024, the Infectious Diseases Working Party (AGIHO) of the German Society for Hematology and Medical Oncology (DGHO) conducted a national survey revealing an increased incidence of PB19V infections across centers. In response, we initiated a retrospective, multi-center, descriptive study of infected patients in Munich, Cologne, and Magdeburg. This report presents one case in detail, including laboratory results throughout the hospital stay, and summarizes additional cases from two institutions across three clinical departments. Anonymized clinical data were collected, including patient demographics, underlying conditions, hemoglobin levels at admission, and other relevant findings. Acute PB19V infection was defined by the detection of PB19V DNA via real-time quantitative PCR (qPCR). In Magdeburg, testing was performed with the RealStar Parvovirus B19 PCR Kit 1.5 (Altona Diagnostics, Cat. No. AS0101543), and in Cologne with the RealStar Parvovirus B19 PCR Kit 1.0 (Altona Diagnostics, Cat. No. 101013); both are CE-IVD-certified commercial kits with predefined primers, probes, and reagents. In Munich, an in-house qPCR assay targeting the NS1 gene (161 bp, nt 2083–2243; NCBI RefSeq NC_000883) was used, with amplification performed using the TaqMan Universal PCR Master Mix (Applied Biosystems). Virological data from all three sites, spanning from 2022 to the end of 2024, were included. Results were reported as genome equivalents per milliliter (Geq/mL) or international units per milliliter (IU/mL), as applicable. Materials tested included serum, saliva, bone marrow, biopsy tissue, and cerebrospinal fluid.
Case presentationsA patient in their 30s presented to the emergency department of LMU University Hospital with general debilitation, fever (up to 39.4 °C), and joint pain. On physical examination, dyspnea and splenomegaly (17.5 × 5.5 cm) were noted. The medical history included heterozygous hereditary spherocytosis (HS). Laboratory tests revealed hemolytic anemia (Hb 6.6 g/dL, bilirubin 8.6 mg/dL, LDH 988 U/L, reticulocytes 102‰, haptoglobin < 0.1 g/L), a CRP of 8.2 mg/L, and a negative Coombs test. Chest X-ray and blood cultures showed no infection. Microbiological testing confirmed a positive PCR result for PB19V, with a viral load exceeding 108 Geq/mL, while serology was initially negative. An aplastic crisis was confirmed by a reticulocyte production index (RPI) < 0.10, and six RBC units were transfused in the first three days. IVIG was not administered. In addition, E. coli was detected in the patient’s urine, leading to a presumptive diagnosis of a urinary tract infection. The patient was treated symptomatically with paracetamol and empiric antibiotics. By day nine post-admission, seroconversion occurred, with both PB19V-IgM and -IgG antibodies turning positive. Two weeks after discharge, her viral load had decreased to 18,000 Geq/mL, and all clinical symptoms had resolved. An RPI of 3.69 indicated active erythropoiesis, with no signs of anemia. Figure 2 (Fig. 2 Laboratory parameters throughout the hospital stay) illustrates the progression of key laboratory parameters during her hospital stay.
Fig. 2
Line graphs illustrating a) hemoglobin (g/dl), b) reticulocyte count, and c) lactate dehydrogenase (LDH) (U/l) of the presented case throughout the hospital stay of 12 days
Facets of PB19V infectionBy correlating clinical severity, hematologic changes, and timing of symptoms with virological findings, we aim to contextualize the subsequent virological analyses and emphasize their clinical relevance. The detailed case (Fig. 2) illustrates the progression of key laboratory and clinical parameters during hospitalization. The summary of additional cases (Tables 1 and 2) captures the broader clinical spectrum of PB19V infection across centers.
In Munich, we observed several severe PB19V cases with heterogeneous presentations (Table 1, Munich_Hem). A patient in their 20s (Munich_Hem1) with HS presented with symptomatic anemia (Hb 5.9 g/dL), requiring four RBC transfusions. The PB19V viral load exceeded 100 million Geq/mL Over the course, the patient developed hepatitis, arthritis, and gastroenteritis, complicating management. In contrast, a teenage patient (Munich_Hem2) also with HS experienced an aplastic crisis with similar hemoglobin levels (5.9 g/dL) but had no inflammatory signs or complications. The patient received two RBC units and was managed as an outpatient. This illustrates that PB19V infection in predisposed individuals can range from mild to severe symptoms. A patient in their 40s (Munich_Hem3) was referred to LMU University Hospital with an acute PB19V infection and a viral load exceeding 100 million Geq/mL, with seronegative status. The case was further complicated by PB19V-triggered hemophagocytic lymphohistiocytosis (HLH), fulfilling 7 of 9 HLH-2004 diagnostic criteria [6]. These included fever, splenomegaly, pancytopenia, hyperferritinemia, elevated sIL-2R, increased triglycerides, and hemophagocytosis observed in bone marrow analysis. Treatment with dexamethasone led to a decline in inflammatory markers and ferritin levels. Subsequently, the patient developed acute kidney failure with nephrotic syndrome, likely secondary to HLH. Additionally, a reactivation of cytomegalovirus (CMV) was observed, with a viral load of 14,000 Geq/mL. The patient discharged herself against medical advice prematurely, and the last measured viral load was 68,000 Geq/ml.
In Cologne (Table 1, Cologne_Hem), a case involved an elderly patient in their 70s (Cologne_Hem1) who presented with a painful, livid skin rash and vasculitis. High PB19V viremia was detected (2.16 million IU/mL), and a skin biopsy confirmed the presence of vasculitis triggered by viral infection. The patient responded well to corticosteroid therapy and his exanthema resolved promptly. In contrast, a younger patient in their 20s (Cologne_Hem3) with CD19 + acute lymphoblastic leukemia post-allogeneic hematopoietic cell transplant, presented with persistent pancytopenia and fever. PB19V viral load reached 27 million copies/mL. IVIG therapy eventually led to clinical stabilization and a reduction in viral load over several weeks. Interestingly, another case demonstrated that anemia is not always a leading symptom of PB19V infection. A patient in their 30s with T-lymphoblastic lymphoma (Cologne_Hem4) presented with a hemoglobin level of 12.7 g/dL and generalized exanthema. Despite persistent PB19V viremia over two months during induction treatment for lymphoma, the patient did not develop anemia.
In Magdeburg (Table 1, Magdeburg_Hem), a patient in their 30s (Magdeburg_Hem1) presented after a recent febrile upper respiratory infection. Immature granulocytes seen by the general practitioner raised concern for acute leukemia, but hematology evaluation revealed normal blood counts. A peripheral smear showed relative monocytosis and plasmacytoid lymphocytes. PB19V DNA was detected at a high level (2,911,500 IU/mL), consistent with a resolving infection; no further diagnostics or treatment were required.
A second case (Magdeburg_Hem2) involved a mid-40s patient with HS, presenting with fatigue, headache, and recent respiratory symptoms. Severe anemia (Hb 4.0 g/dL) with tachycardia was due to hemolysis from acute PB19V infection (13,423,750 IU/mL) and folate deficiency. The patient received five units of RBCs and folate supplementation. At follow-up 19 days later, the patient had clinically improved, hemoglobin rose to 10.5 g/dL, and viral load declined to 420,250 IU/mL, with residual mild hemolysis attributable to the underlying condition.
Next, we focused on children and adolescents and gathered a series of compelling cases (Table 1, Munich_Ped). One case involved a preschool-aged child with sickle cell disease (Munich_Ped1) who presented with severe anemia (Hb 5.0 g/dL), fever, and a vaso-occlusive crisis. The patient required a transfusion, and PB19V PCR revealed a significantly elevated viral load (> 100 million Geq/mL). Another middle childhood patient with DiGeorge syndrome, a T-cell immunodeficiency (Munich_Ped3), presented with fever, cervical lymphadenopathy (LAD), and mild anemia (Hb 10.7 g/dL). Despite a high viral load (> 100 million Geq/mL) and positive IgM antibodies, the patient did not require a transfusion. In this case, a lymph node biopsy was performed to rule out lymphoproliferative disorders, given the predisposition associated with Di-George syndrome and underlying immune deficiencies. Another school-aged child (Munich_Ped4) previously healthy and diagnosed with IgA vasculitis presented with purpura, fever, abdominal pain, and mild thrombocytopenia but stable hemoglobin levels (12.2 g/dL), requiring no transfusion. Elevated PB19V PCR and positive IgG and IgM antibodies confirmed the association between PB19V and vasculitis. Lastly, a pre-school aged child with iron deficiency anemia (Munich_Ped5) presented with critically low hemoglobin (Hb 2.4 g/dL), fever, and mild thrombocytopenia, and no further symptoms. The patient required a transfusion, and PB19V PCR revealed a viral load of 9 million Geq/mL, with positive IgG and IgM antibodies further complicating the clinical picture of pre-existing anemia.
Table 1 Overview of the diverse clinical presentations of PB19V infection in hematology and pediatricsEach row represents an individual patient case from the hematology and pediatric departments in Munich (Munich_Hem, Munich_Ped), as well as from the hematology department in Cologne (Cologne_Hem) and Magdeburg (Magdeburg_Hem). Columns show key aspects including, site of care, comorbidities, age group, hemoglobin levels, number of transfusions, and clinical presentation.
In the gynecology department of the LMU University Hospital, several cases highlight the severe risks associated with PB19V infection during pregnancy (Table 2, Munich_Gyn). A woman in her 30s (Munich_Gyn1) presented for first-trimester screening at 11 + 6 weeks of gestation. Although asymptomatic, she had been diagnosed with a PB19V. The scan revealed an increased nuchal translucency (5.6 mm), but the fetus appeared otherwise normal. Six days later, during a planned amniocentesis, no fetal cardiac activity was detected. The fetus was delivered at 13 + 0 weeks following miscarriage induction. Another case involved a woman in her 20s at 28 + 4 weeks of gestation (Munich_Gyn2), who experienced intrauterine fetal death, presenting with absent fetal movements. A recent PB19V infection, likely contracted before 20 weeks of pregnancy, was identified. Despite no abnormalities observed on autopsy or placental histology, significant fetal anemia caused by the infection was suspected as the primary cause of death. Case Munich_Gyn4 illustrates a favorable outcome with the birth of a healthy newborn following successful intrauterine blood transfusions. Nevertheless, it is crucial to consider the implications of PB19V infection in younger populations. Children under three years of age demonstrate low immunity to PB19V and many infected children remain asymptomatic. The rising number of infections places seronegative pregnant women at increased risk, particularly those with young children in their household (3).
Table 2 Overview of the diverse clinical presentations of PB19V infection in pregnant womenVirological analysesAs in most European Union countries, PB19V infections are not subject to systemic surveillance in Germany. There is no nationwide reporting obligation under the Infection Protection Act (IfSG), resulting in a lack of epidemiological data on incidence and seroprevalence. To address this gap and improve data visibility, we present virological data from Munich, provided by the Max von Pettenkofer Institute (MvP), and from Cologne and Magdeburg contributed by their respective virology departments. Between January and December 2024, a total of 936 qPCR tests for PB19V were conducted by the MvP. Strikingly, the number of positive cases increased markedly, with the first quarter of 2024 alone exceeding the total annual number of positives recorded in previous years. Specifically, 48 PCR tests returned positive results in the first quarter, corresponding to a patient-based positivity rate of 16%, followed by a rate of 18.2% in the second quarter. A sharp decline in positivity was observed in the third and fourth quarters, dropping to 1.2%. For comparison, in 2023, only 15 of 641 PCR tests were positive for PB19V, yielding a positivity rate of 2.3%. In the first quarter of 2025, we observe an even lower positivity rate of 0.8%, reflecting reduced transmissions following prior population exposure. However, factors such as seasonal variation and reduced testing intensity post-peak may also contribute to this trend, and definitive conclusions regarding herd immunity require supporting seroprevalence data. Interpretations remain challenging, as individual infection courses are largely unavailable. Notably, the overall testing volume per quarter tripled in 2024 compared to the previous year. This upward trend in PB19V detection is further supported by virological data from the University Hospitals of Cologne and Magdeburg (Fig. 3 Number of positive PB19V PCR tests (total numbers) per medical specialty in Munich). At all three centers, most infections were acute and characterized by high viral loads (Fig. 4 PB19V-DNA peak levels in positive patients during 2024 in Munich, Cologne, and Magdeburg). The majority of test submissions originated from pediatrics (40.8–66.7%), followed by hematology. At Otto von Guericke University Magdeburg, all submitted cases were from the hematology department. At LMU University Hospital Munich, a notable number of cases originated from gynecology (21.4%). This distribution reinforces the identification of particularly vulnerable populations affected by PB19V. Additionally, departments such as gastroenterology and nephrology/rheumatology also contributed a significant number of positive cases, suggesting that PB19V may play a role in complicating conditions in these specialties. Smaller numbers of cases were reported from dermatology, otolaryngology, infectiology, and pulmonology, indicating that while PB19V may be less frequently encountered in these fields, it still presents in a broad range of clinical scenarios (Fig. 5 Number of positive PB19V PCR tests (total numbers) per medical specialty in Munich, Cologne, and Magdeburg).
Fig. 3
Total number of positive PCR test results (from any material) from 2022 to 2024 across three sites: Cologne, Magdeburg, and Munich. Only one positive test per patient was counted
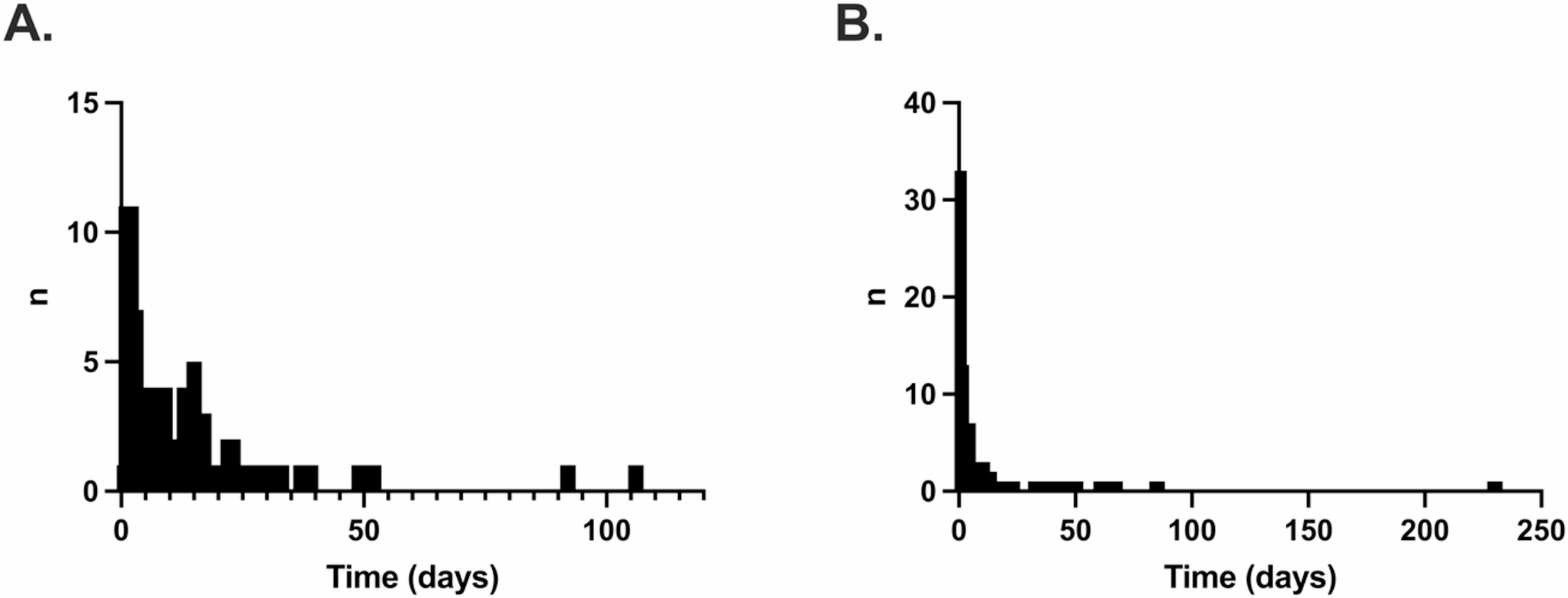
Fig. 4
Each dot represents the highest measured PB19V DNA level for an individual PCR-positive patient, all measured in blood samples. Data from Munich (n = 116) are shown in Geq/mL, while data from Cologne (n = 56) and Magdeburg (n = 10) are presented in IU/mL. Red horizontal lines indicate the geometric mean, and vertical red bars show the 95% confidence interval. Dotted black lines represent the lower detection limit (102) and the upper saturation threshold (108)
Fig. 5
Pie chart displaying the distribution of PB19V PCR test submissions by medical specialty at the LMU University Hospital and the Cologne University Hospital. Submitting departments include pediatrics, gynecology, hematology, gastroenterology, rheumatology, emergency, surgery, pulmonology, otolaryngology, dermatology, and cases categorized as not applicable (N/A)
Comments (0)