
Remember me
CTCs are cancer cells released from a primary tumor or metastatic site into the bloodstream. These cells are critical in the metastatic cascade, potentially leading to the formation of secondary tumors in distant organs. First identified over 150 years ago, CTCs are valuable biomarkers for understanding tumor biology, predicting metastasis, and monitoring disease progression [13]. CTCs are rare in the bloodstream, often found at concentrations as low as one CTC per 10⁶–10⁸ leukocytes. Their rarity, combined with a high background of normal blood cells, poses significant challenges to their detection and isolation. Accordingly, highly sensitive and specific enrichment methods have been developed to address these hurdles [14].
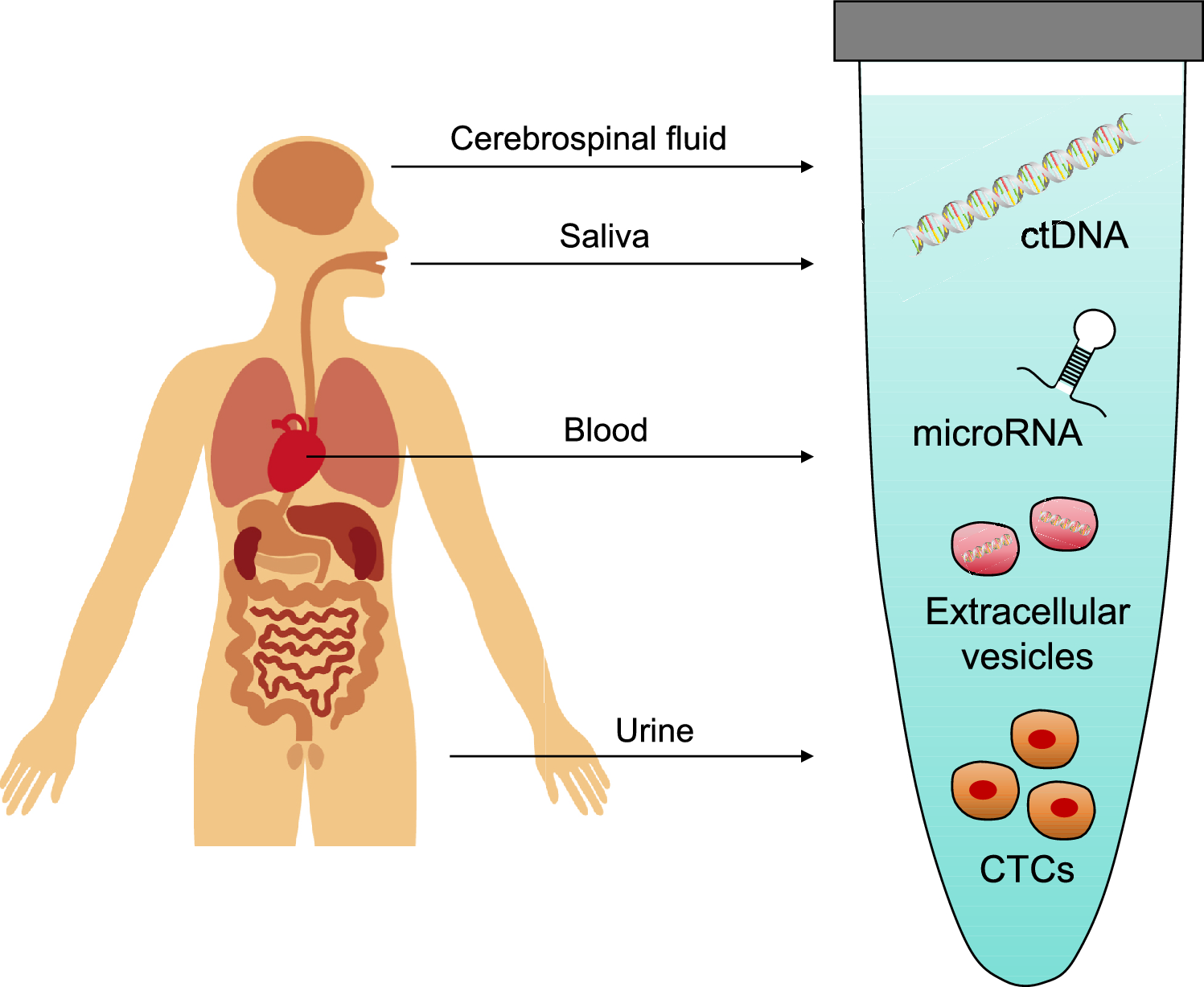
CTC enrichment methods are developed based on the physical and biological properties of these cells [15, 16]. For example, size-based isolation techniques, such as the isolation by size of tumor cells method, separate CTCs based on their larger size compared with normal blood cells. Advanced systems like the MetaCell kit, which uses an 8 µm porous membrane, and CellSieve™ filters [17], which employ size-exclusion principles, have demonstrated efficacy in isolating CTCs from patients with various sarcoma subtypes, including osteosarcoma, chondrosarcoma, and rhabdomyosarcoma (Table 1). These antibody-independent options makes them particularly useful for capturing CTCs from sarcomas, where specific surface markers are not well characterized [18]. However, these methods are limited: white blood cell retention on microfiltration membranes can cause contamination, and smaller CTCs may escape capture, reducing the overall efficiency [19]. To overcome these limitations, innovative strategies to increase the CTC cluster size, such as selective size amplification using antibodies or binding agents, can improve capture rates and detection precision (Fig. 1).
Table 1 The CTC detection in patients with bone and soft-tissue sarcomasFig. 1
Circulating molecular targets used in liquid biopsy
Biological detection methods utilize tumor-associated surface proteins to identify CTCs. For example, the CellSearch system, the first FDA-approved technology for CTC detection, targets cells expressing the epithelial cell adhesion molecule (EpCAM) [20]. While effective for epithelial-origin cancers such as breast, colorectal, and prostate cancers, this method does not detect sarcomas, of mesenchymal origin. Alternative markers, such as cell surface vimentin, have been explored for sarcomas [21]. In addition, immunomagnetic separation techniques using markers such as CD99 for Ewing sarcoma [22] have demonstrated high viability in isolating functional CTCs.
RNA-based detection methods also provide options for distinguishing sarcoma cells from normal blood cells. These techniques rely on the unique gene expression profiles of sarcoma CTCs, such as EWS-FLI1 fusion transcripts in Ewing sarcoma, to ensure accurate identification. The detection of EWS-FLI1 fusion-positive CTCs has provided a valuable tool for early diagnosis, monitoring minimal residual disease (MRD), and predicting recurrence of Ewing sarcoma [23]. In osteosarcoma, CTCs expressing mesenchymal markers such as CSV or osteoblastic markers such as alkaline phosphatase [24] have been correlated with disease progression. In soft-tissue sarcomas, including leiomyosarcoma, synovial sarcoma, and liposarcoma, CTCs present unique challenges due to tumor heterogeneity [25]. Epidermal growth factor receptor (EGFR) positivity in CTCs has been observed in up to 93.75% of high-grade cases, suggesting the possibility of developing targeted therapies against EGFR [26]. In rhabdomyosarcoma, CTCs often display myogenic markers such as desmin and MyoD1, which may assist in their isolation and characterization.
Advances in CTC detection and enrichment technologies have enabled their capture and analysis, offering insights into tumor biology, metastasis, and therapeutic response. Despite current challenges such as heterogeneity among sarcoma subtypes and technical limitations in CTC isolation, ongoing research aims to refine these methodologies [27]. Although liquid biopsy targeting CTC has not yet achieved to clinics, integrating CTC analysis into routine clinical practice holds the potential to revolutionize sarcoma care.
Circulating tumor DNA (ctDNA)ctDNA comprises DNA fragments released into the bloodstream during tumor cell apoptosis, necrosis, or active secretion [28]. These fragments carry tumor-specific genetic and epigenetic alterations, providing noninvasive and dynamic insights into the tumor genome. Compared with traditional tissue biopsy, ctDNA analysis offers several advantages, including the ability to capture tumor heterogeneity, monitor real-time changes in tumor dynamics, and assess therapeutic efficacy.
Technologies for ctDNA detection include droplet digital PCR (ddPCR) [29] and next-generation sequencing (NGS) [30]. ddPCR provides high sensitivity and specificity, enabling detection of low-frequency mutations. This is particularly useful for monitoring specific mutations in sarcoma-related genes such as TP53 and RB1, commonly altered in bone and soft-tissue sarcomas (Table 2). NGS, conversely, allows comprehensive genomic profiling, including detection of multiple mutations, copy number variations, and structural rearrangements. This comprehensive approach is invaluable for identifying actionable targets and informing personalized treatment strategies.
Table 2 The ctDNA detection in patients with bone and soft-tissue sarcomasIn the osteosarcoma biology study by the Children Oncology Group, an ultra-low-pass whole-genome sequencing assay in 72 patients with primary localized osteosarcoma detected ctDNA in 57% of newly diagnosed patients with osteosarcoma; further, the risk of events and death increased with ctDNA levels [31]. Another study using plasma samples from the prospective OS2006 trial used an ultra-low-pass whole-genome sequencing assay to detect copy number alteration in 183 patients. While the metastatic status at diagnosis is the main known prognostic factor in osteosarcoma, Audinot et al. reported that the copy number abnormality score at diagnosis (diagCPA) is a continuous variable independently associated with outcomes [32]. diagCPA was also a major prognostic factor at the time of surgery and until the end of treatment, independent of the histological response [32]. These data indicate that adding diagCPA to the metastatic status at diagnosis or poor histological response after surgery improves prognostic stratification.
Ewing sarcoma is characterized by the presence of EWSR1 rearrangements with a member of the ETS family of genes [33]. The two most common fusion genes are EWSR1-FLI1 and EWSR1-ERG, which occur in 85–90% and approximately 10% of cases, respectively [34, 35]. In the EWING2008 trial, genomic EWSR1 fusion sequence spanning primers and probes were used for ctDNA quantification by digital droplet PCR in plasma samples from 102 patients with Ewing sarcoma. Accordingly, Krumbholz et al. reported that pretreatment ctDNA copy numbers correlated with event-free and overall survival. Interestingly, decreased ctDNA levels were observed in most cases after only two blocks of induction chemotherapy consisting of vincristine, ifosfamide, doxorubicin, and etoposide [36]. Recently, Sulman et al. demonstrated that a ctDNA burden ≥ 0.5% after one cycle of chemotherapy can identify patients highly likely to relapse, which may contribute to novel risk-adapted therapy trials focused on ctDNA burden [31].
ctDNA detected in other types of sarcoma include the IDH1/2 mutation in chondrosarcoma [37], t(X;18)(p11;q11) in synovial sarcoma, which fuses SS18 in chromosome 18 to SSX1 or SSX2 in chromosome X [38], and PAX3-FOXO1 fusion in rhabdomyosarcoma [39]. In leiomyosarcoma, ctDNA analysis has uncovered frequent mutations in ATRX and TP53, associated with poor outcomes [40].
Despite its potential, ctDNA analysis faces several challenges in sarcoma. The low ctDNA concentration in the bloodstream, especially in sarcomas with low cellular turnover, requires the use of highly sensitive detection methods. Further, the heterogeneity of bone and soft-tissue sarcomas complicates ctDNA analysis, as a single mutation may not fully represent the molecular landscapes of the tumor. Multi-gene panels and whole-genome sequencing are emerging as potential solutions to better capture the complexity of sarcoma genomes.
Circulating microRNAmicroRNAs (miRNAs) are small noncoding RNA molecules with approximately 18–25 nucleotides that modulate the expression of multiple target genes, playing important roles in various physiological and pathological processes [41,42,43,44]. Reportedly, miRNAs are frequently upregulated or downregulated in various tumors, indicating that miRNAs act either as oncogenes or tumor suppressors [45, 46]. A previous report showed that tumor cells secrete miRNAs into the circulation [47]. Their high stability and tissue specificity arise from their encapsulation within extracellular vesicles, such as exosomes or microvesicles, or their association with lipoprotein complexes [45]. Since then, the analysis of circulating miRNA levels in serum or plasma has been considered a novel approach in liquid biopsy, with significant potential for diagnosis, monitoring, and prognosis of bone and soft-tissue sarcomas (Table 3).
Table 3 The ctRNA detection in patients with bone and soft-tissue sarcomasNumerous studies have been conducted on the circulating miRNA signatures in osteosarcoma [48]. For instance, miR-21, an oncogenic miRNA, is significantly overexpressed in blood samples of patients with osteosarcoma, being associated with a worse prognosis. Other miRNAs upregulated in patients’ blood include miR-25-3p, miR-29 family, miR-191, miR-196, miR-421, and miR-542-3p [49,50,51,52,53,54] (Table 3). Among these, miR-25-3p has an oncogenic function intracellularly and extracellularly, with a negative correlation between expression levels and the prognosis of patients with osteosarcoma [49, 55]. In contrast, miR-34a, which is downregulated in osteosarcoma tissues, is underexpressed in blood samples, and associated with advanced disease [52]. Similarly, circulating miR-143, miR-199a-3p, miR-101, miR-206, miR-124, and miR-497 are downregulated in patients with osteosarcoma [56,57,58,59] (Table 3). Circulating miR-320a levels are higher in the osteoblastic than in the chondroblastic subtype, whereas circulating miR-199a-3p levels were significantly low in the osteoblastic subtype [60]. In patients with Ewing sarcoma, serum miR-125b expression is decreased compared with that in healthy individuals [61]. Interestingly, patients with a poor response to chemotherapy showed a significant miR-125b downregulation (Table 3).
In patients with dedifferentiated liposarcoma, miR-1246, -4532, -4454, -619-5p, and -6126 are highly expressed in human dedifferentiated liposarcoma cell lines, tissues, serum, and exosomes, and can be used as biomarkers for early diagnosis or treatment targets [62]. Rhabdomyosarcoma, the most common soft-tissue sarcoma in childhood, shows high expression levels of muscle-specific miRNAs (miR-1, miR-133a, miR-133b, and miR-206). In their analysis of muscle-specific miRNA levels in the blood serum of patients with RMS, Miyachi et al. found that normalized serum miR-206 exhibited the highest sensitivity and specificity among muscle-specific miRNAs [63]. Approximately 50% of MPNSTs, which typically originates from cells forming the nerve sheath such as Schwann and perineural cells, occur sporadically and the rest of them originate in patients with the autosomal dominant genetic disorder neurofibromatosis type 1 (NF-1). Weng et al. found higher miR-801 and miR-214 expression in the serum of sporadic MPNST patients and NF1 MPNST patients than in NF1 patients [64]. Moreover, miR-24 was significantly upregulated in NF1 MPNST patients. Therefore, combining the three miRNAs (miR-801, miR- 214, and miR-24) could serve to distinguish NF1 MPNST patients from NF1 patients [64].
Although circulating miRNA detection technologies face challenges related to sensitivity, specificity, and standardization, future research will focus on combining circulating miRNAs with other liquid biopsy markers such as ctDNA and extracellular vesicles to improve diagnostic accuracy [65]. Along with improvements in detection technologies, circulating miRNAs have a potential in the revolution of the management of bone and soft-tissue sarcomas, paving the way for personalized oncology.
Circulating microvesiclesExtracellular vesicles (EVs) are small vesicles, 50 nm to 2 μm in size, released from the surface of several cell types into bodily fluids such as blood, saliva, milk, sweat, tears, and urine [66]. There are several classes of EVs, including exosomes, microvesicles, and apoptotic bodies, produced by different mechanisms. EVs play a critical role in intercellular communication by transferring biomolecules such as proteins, lipids, mRNA, and miRNA between cells. In the tumor microenvironment, EVs secreted by tumor cells can interact with surrounding cells, delivering biomolecules to influence processes like tumor growth, invasion, metastasis, and chemotherapy resistance [67]. EVs are small membranous vesicles composed of a lipid bilayer with a cystic structure and high molecular stability in body fluids. Recently, EVs have received considerable attention as a target of liquid biopsy. Since EVs express tetraspanin family proteins such as CD63, CD81, and CD9 [68, 69], circulating EVs could be detected by these proteins as well as other tumor-specific markers.
In their proteomic analysis of purified EVs from synovial sarcoma (SS) cell lines, Yokoo et al. identified 199 common proteins across EVs. Among them, monocarboxylate transporter 1 (MCT1) was identified as a surface marker of SS-derived EVs, highly expressed in SS patient-derived EVs compared with healthy individuals (Table 4) [70]. Most importantly, the serum levels of MCT1+ CD9+ EVs reflect the tumor burden in SS patients. Interestingly, positive MCT1 was observed in most SS specimens and its cytoplasmic/plasma membrane expression was significantly associated with worse overall survival, indicating the potential therapeutic target.
Table 4 The Detection of extracellular vesicles in patients with bone and soft-tissue sarcomasUotani et al. identified ENO-1 and CD99, a marker for the immunohistochemistry of ES, on EVs purified from the blood serum of patients with Ewing sarcoma before treatment (Table 4). In an animal model of Ewing sarcoma, ENO-1+ CD63+ EVs were elevated along with tumor growth and reduced after tumor resection. Importantly, increased ENO-1+ CD81+ EVs in the patient serum before treatments can distinguish patients with Ewing sarcoma from healthy individuals with an area under the curve of 0.92 and reflected the tumor burden in Ewing sarcoma patients during multidisciplinary treatments [71].
Since EVs contain genetic material such as mRNA, miRNA, or DNA [72], advances in high-throughput technologies such as exosomal RNA sequencing and proteomic profiling, will enable more comprehensive analyses of exosomal cargo, which may identify specific molecular markers for a various malignant diseases. Combining exosome analysis with other liquid biopsy targets, such as ctDNA and CTCs, could improve diagnostic accuracy and provide a comprehensive view of tumor dynamics. Of note, EV-based delivery systems are being explored for targeted therapies, leveraging their natural ability to transfer therapeutic agents directly to tumor cells [73].
Comments (0)