
Remember me
The number of patients undergoing dialysis and receiving cancer pharmacotherapy is increasing. A multicenter retrospective study conducted in Japan reported that the median overall survival of patients receiving palliative chemotherapy was 13 months, whereas the 3-year survival rate of patients receiving perioperative chemotherapy was 79% [16]. This finding suggests that with appropriate assessment of the patient’s condition and dosage adjustment, effective and safe cancer pharmacotherapy may be feasible, even in patients undergoing dialysis.
In patients undergoing dialysis, although renal function is markedly impaired, hepatic and other physiological functions are not necessarily compromised. Therefore, designing rational dosing regimens for this population is often feasible. In particular, understanding whether a drug is removed by dialysis is useful for determining appropriate dose adjustments. The extent to which a drug is cleared by dialysis depends on its molecular weight, water/lipid solubility, protein binding, and volume of distribution [17, 18]. In general, drugs with a low molecular weight, high water solubility, and low protein binding are more likely to be removed by dialysis. Conversely, lipophilic drugs typically possess a large distribution volume and high tissue permeability; therefore, they are less likely to be removed from the blood, and the efficacy of dialysis in clearing such drugs is limited. For example, among the platinum-based drugs, cisplatin has a large distribution volume and high tissue penetration; therefore, its removal by dialysis is minimal [19]. In contrast, carboplatin has a relatively smaller volume of distribution and is partially removed by dialysis [20]. Furthermore, the drug clearance per unit time achieved by dialysis may exceed the patient’s native renal clearance. As a result, blood concentrations may decrease rapidly during dialysis, followed by a rebound increase owing to redistribution from peripheral tissues into the blood.
On the other hand, even drugs for which the kidneys do not play a major role in metabolism or inactivation may exhibit pharmacokinetic profiles that differ from those in patients with normal renal function. 5-Fluorouracil (5-FU) is primarily eliminated by the liver; thus, renal function is considered to have little effect on its pharmacokinetics or efficacy (Fig. 2). However, recent reports have shown that in patients with impaired renal function, especially those undergoing dialysis, the metabolites of 5-FU, fluoro-β-alanine (FBAL) and fluoroacetate (FA), can accumulate after administration [21]. Furthermore, patients undergoing dialysis may have an increased risk of hyperammonemia associated with 5-FU treatment [22,23,24]. The toxicity associated with these metabolites is thought to occur via mechanisms distinct from those of 5-FU. 5-FU is mainly metabolized by dihydropyrimidine dehydrogenase, including an initial conversion to dihydrofluorouracil, then to fluoroureidopropionic acid, and subsequently to FBAL. FBAL is further metabolized into compounds such as FA, and some of these water-soluble metabolites can be eliminated by the kidneys (Fig. 2A). It is estimated that over 80% of administered 5-FU undergoes this metabolic pathway [21]. Therefore, attention should be paid to the potential accumulation of these metabolites in patients with significantly impaired renal function (Fig. 2B). Recent reports have suggested that adjusting the timing of dialysis may help reduce metabolite accumulation and prevent adverse effects. For example, when 5-FU is administered as a 48 h continuous infusion, dialysis on the day following the start of administration may help reduce the accumulation of 5-FU metabolites and the risk of hyperammonemia [23].
Fig. 2
Metabolic pathways of 5-fluorouracil (5-FU). A 5-FU is mainly metabolized in the liver by dihydropyrimidine dehydrogenase (DPD), initially converting to dihydrofluorouracil (FUDH), then to fluoro-ureidopropionic acid (FUPA), and subsequently to FBAL. FBAL is eliminated by the kidneys but can be further metabolized into fluoroacetate (FA). Over 80% of administered 5-FU undergoes this metabolic pathway. B In patients with significantly impaired renal function, renal clearance of FBAL would be significantly decreased, and caution is required regarding the accumulation of FBAL or FA
Because renal excretion is a major pathway for eliminating platinum, Ccr and the clearance of plasma ultrafilterable platinum (fPt) are significantly correlated in patients administered oxaliplatin. Thus, when a constant dose is administered, regardless of renal function, the AUC of fPt increases with decreasing renal function. However, this increase in fPt is not correlated with the incidence or severity of adverse events [25]. One possible explanation for these results is that fPt in the plasma consists of a mixture of reactive platinum species capable of binding to biological molecule, such as DNA and inactive platinum species that have lost their reactivity [26]. Therefore, renal function may have a limited effect on the elimination of pharmacologically reactive platinum (Fig. 3A). In our study using an animal model, we found that plasma concentrations of DNA-reactive platinum declined rapidly after oxaliplatin administration, regardless of renal function [27]. Moreover, in a patient undergoing dialysis with advanced gastric cancer treated with mFOLFOX7, total platinum and fPt concentrations decreased to approximately 35.9% and 7.3%, respectively, on days 2 and 14, respectively, post administration. In contrast, the DNA-reactive fPt had already decreased to 1.9% and 0.6%, respectively, at the same time points, indicating more rapid elimination. These findings suggest that pharmacologically reactive platinum, which is responsible for both therapeutic efficacy and toxicity, may be rapidly cleared from the body, regardless of renal function. Indeed, although high levels of platinum exposure have been observed in patients undergoing dialysis and receiving oxaliplatin, the treatment is generally well-tolerated [28, 29]. These findings underscore the importance of evaluating not only the pharmacokinetics of the parent drug, but also those of its metabolites, including their accumulation and potential bioactivity, when optimizing pharmacotherapy in this population (Fig. 3B, C).
Fig. 3
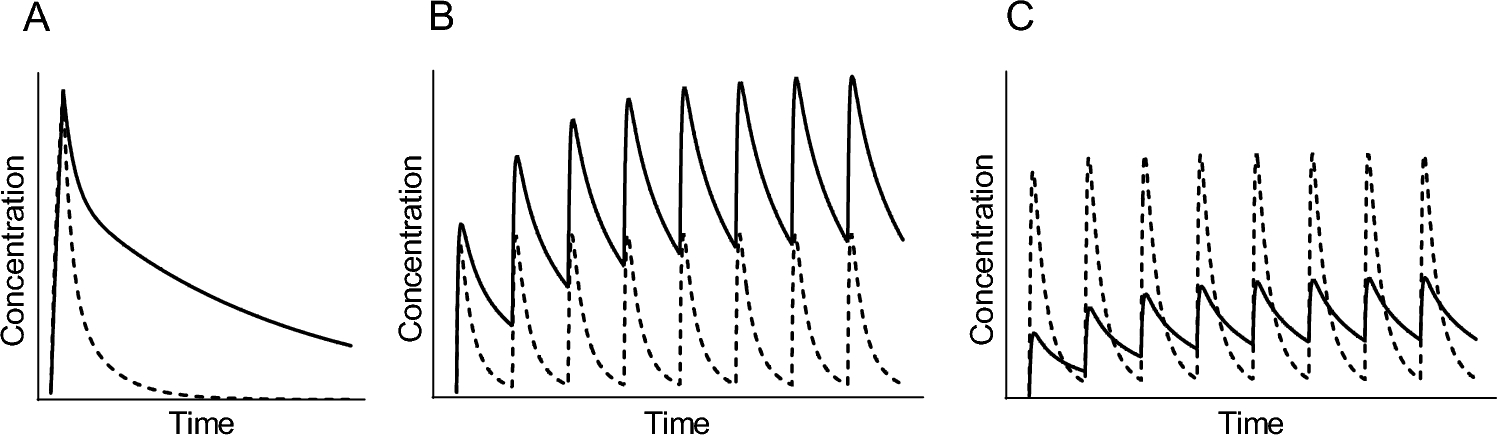
Pharmacokinetic profiles of oxaliplatin in patients undergoing dialysis. A In patients administered oxaliplatin, plasma ultrafilterable platinum (fPt) consists of a mixture of reactive platinum species capable of binding to biological molecules, such as DNA, and inactive platinum species that have lost their reactivity. The decline in the plasma concentration of reactive fPt is thought to occur primarily through a non-enzymatic conversion to inactive species or through distribution into peripheral tissues. B, C Assuming a drug like oxaliplatin, for which the kidneys play only a minor role in metabolism or inactivation, but whose metabolites are primarily excreted renally, changes in blood concentrations following a single dose can be predicted. The solid line represents the parent compound, while the dashed line represents the metabolite. Compared to a patient with normal renal function (B), a patient with impaired renal function (C) is expected to show a gradual increase in blood levels of the metabolite after administration. A similar trend is expected not only with bolus injection, but also during constant-rate intravenous infusion
Comments (0)