As the intensity of the NAC for EC increased from doublet to triplet regimen, significantly higher incidences of severe adverse events were observed in DCF regimen than found with the former CF regimen [6]. Accordingly, the negative impact of DCF on preoperative nutritional status and skeletal muscle loss could be considered to a greater degree than observed with the former neoadjuvant CF. In addition, the Japanese EC practice guidelines also mention that administration of neoadjuvant DCF can be too intense in some patients, especially in those who are elderly and patients with various severe comorbidities [7]. A previous study also reported that DCF was superior to the CF regimen in long-term survival, while the survival benefit of DCF was not observed in patients ≥ 76 years [18]. In such situations, two courses of DCF, rather than the normal three courses, could become an additional clinical option. Moreover, Kubo et al. mentioned that continuing the third course of neoadjuvant DCF even had a risk of worsening survival in patients who did not experience a response to the prior two courses of DCF in locally advanced EC [19].
This study focused on the differences in the influences of the two and three courses of DCF on nutritional status and skeletal muscle change during neoadjuvant treatment. Our findings showed that two major nutrition-related indicators, PNI and GNRI, were significantly decreased during the NAC treatment in the three-course DCF and relatively maintained in the two-course DCF. Similarly, compared with two courses of DCF, three courses had a negative effect on the skeletal muscle volume during NAC. Furthermore, multivariate analysis showed that three courses of DCF was an independent risk factor for the rates of changes in PNI, GNRI, and PMA. On the contrary, there was no significant difference in NLR between the two groups, which might be because several patients experienced neutropenia as an adverse event of chemotherapy and required subsequent use of granulocyte colony stimulating factor. Similarly, no significant difference was observed in their GPS changes. This lack of an effect of the difference between two- and three-course DCF on the GPS changes could be because the crude cutoff setting that was designed for a screening method made it difficult to reveal the difference. When comparing hematological adverse events, neutropenia with CTCAE grade ≥ 2 was significantly higher in the three-course than the two-course group. The survival analysis showed no significant difference between the two-course and three-course groups in any pStage. Although it was difficult to completely avoid bias related to the differences in the patients’ backgrounds between the two groups, our findings indicated that the three-course DCF regimen was inferior to the two-course regimen, especially with respect to the nutritional status and skeletal muscle loss.
Our univariate and multivariate analyses for multiple indicators showed other interesting findings. Although three courses of DCF had negative effects on PNI and GNRI, low nutritional status with a PNI < 45 at the initial diagnosis was positively associated with the change rates of PNI and GNRI. These findings indicated that patients with good nutritional condition can be more susceptible to NAC than those who are persistently malnourished due to EC conditions. We usually consider providing nutritional support for patients who are malnourished, however, even the patients in good nutritional condition can have a risk of nutritional disorder when receiving intense neoadjuvant treatment.
Several previous studies have reported the clinical importance of nutritional support during neoadjuvant treatment [20, 21], and multiple previous studies have shown that the skeletal muscle loss even during NAC was associated with postoperative complications and reduced long-term survival [22,23,24]. EC is prone to causing nutritional disorders due to the tumor’s location and requires a long treatment period from the initial diagnosis to radical esophagectomy that is highly invasive; therefore, treatment strategies that can maintain nutritional status and skeletal muscle volume are essential. Our results showed that two courses of DCF should be considered as a treatment option.
We should note that our results do not support recommending two courses of neoadjuvant DCF in all patients. The strongest evidence of the superiority of DCF to CF in NAC for locally advanced EC was primarily based on the JCOG 1109 study with three courses of DCF. Regarding tumor shrinkage achieved by radical surgery and reduction of postoperative recurrence due to control of micrometastases, three courses of DCF was considered to have a greater clinical benefit than two courses, except for DCF-resistant EC. In clinical practice, the number of administered courses should be comprehensively determined according to the clinical situation, including the patient’s overall condition and degree of cancer progression; however, when considering the highly negative effect of three courses on nutritional status and skeletal muscle loss, more aggressive intervention to prevent malnutrition and sarcopenia during neoadjuvant treatment is essential when three courses of DCF are administered as NAC.
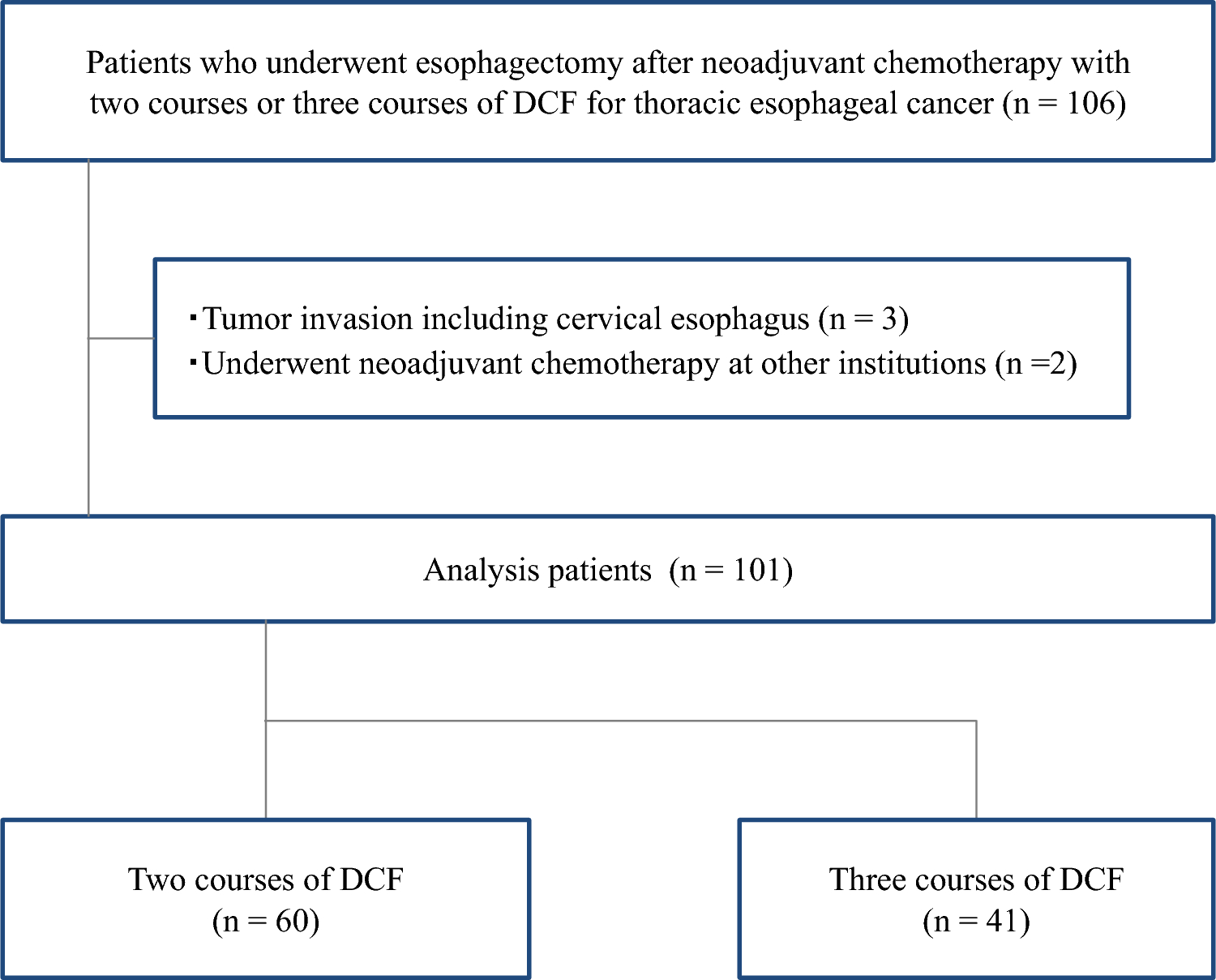
This study had several limitations. First, the biases due to the retrospective study design, especially in the patients’ characteristics, could not be avoided. Actually, although administration of two or three courses was only related to whether or not the treatment was given in the early or later study period, some patients with highly advanced EC, such as Stage IV EC, received three courses even in the later study period. This bias probably influenced the patient characteristics, particularly the cancer stage. To minimize the influence of these limitations, this study reviewed all patients who underwent esophagectomy after neoadjuvant DCF during the study period to evaluate the factors that had effects on reduced nutritional status and greater skeletal muscle loss by performing multivariate analysis. Moreover, in the analysis of long-term survival, the analysis was stratified by pStage. Second, nutritional status and skeletal muscle volume were evaluated only from blood-test data and computed tomography images, respectively, in this study. Malnutrition and skeletal muscle loss resulting in sarcopenia should be assessed by multiple measures, including body composition, physical assessment (such as muscle strength and gait speed), history of oral intake, and daily activity status; therefore, detailed assessment of the influence of NAC on sarcopenia was difficult. However, these indicators, including PNI, GNRI, and PMA, are useful and typical measures that are easy to measure in clinical settings. It is easy to confirm reproducibility, and further clinical research and applications are expected in the future. Third, the risk of selection bias as this was single-center study could not be excluded. The study sample size was not large, and the management of NAC for EC probably varies among institutions; therefore, generalizing from our comparison of two-course and three-course DCF based only on our findings is probably unwarranted without additional supportive studies. Despite these limitations, we believe that our findings provide important information from a new perspective related to novel NAC using DCF regimen.
In conclusion, this study showed that worsening of nutritional status and greater skeletal muscle loss during NAC were more serious with three courses than with two courses of neoadjuvant DCF. If only considering the effects of nutritional status and skeletal muscle volume, our results showed that two courses were superior to three courses of neoadjuvant DCF.

Comments (0)