
Remember me





Over the past decade, the use of radiological imaging in forensic medicine has increased considerably. Radiological techniques offer significant advantages in the evaluation of postmortem cases. For instance, multi-detector computed tomography (MDCT) provides comprehensive visualization of soft tissues, the skeleton, and internal organs without the need for invasive manipulation of the body prior to autopsy [1]. Furthermore, the administration of contrast medium via minimally invasive cannulation of the femoral vessels, as performed in multi-phase postmortem CT angiography (MPMCTA) [2, 3] enables detailed assessment of the vascular system. This imaging modality is, therefore, a valuable complementary and preparatory tool for autopsy procedures.
However, MDCT has certain limitations, particularly due to its low intrinsic soft tissue contrast, which reduces its effectiveness in evaluating solid organs and soft tissues such as the liver, musculature, and nervous system. This limitation is not observed with magnetic resonance imaging (MRI), which offers superior contrast resolution for these structures. While image contrast remains largely unchanged between clinical and postmortem images obtained with MDCT, postmortem magnetic resonance imaging (PMMR) often reveals notable differences in contrast, enhancing the visualization of anatomical and pathological details. Studies [4,5,6,7,8,9,10,11] indicate that changes in the relaxation times (T1 and T2) of soft tissues, organs, and bone marrow can impact the various contrast images encountered in PMMR. Nevertheless, PMMR has already been implemented in the routine daily practice of several forensic centers. Most of the PMMR protocols currently in use are based on clinical radiology practice and have been modified to closely align with established clinical standards.
Despite the possible changes in the contrast-image, informed radiologists can analyze these postmortem images for all sequences without encountering issues. One notable exception is the fluid-attenuated inversion recovery (FLAIR) sequence, which is known to perform poorly in cases involving low body temperature [12]. Quantitative assessments in postmortem imaging, such as brain or myocardial mapping and the Apparent Diffusion Coefficient (ADC) measurements, must be interpreted carefully, as postmortem changes can influence their reliability and diagnostic value [13,14,15,16].
In clinical radiology, FLAIR sequence, whether 2D or 3D, is commonly used in brain imaging to detect signs of multiple sclerosis, suspected child abuse (non-accidental head injury), inflammation or infection (e.g., encephalitis, herpetic infection), stroke, or acute bleeding. In this sequence, the signal from cerebrospinal fluid (CSF) is suppressed by applying a specific inversion time (TI) that corresponds to the longitudinal relaxation time of CSF [17,18,19]. Even in clinical settings, interpreting FLAIR images can be challenging, as factors such as dehydration can influence image quality [20].
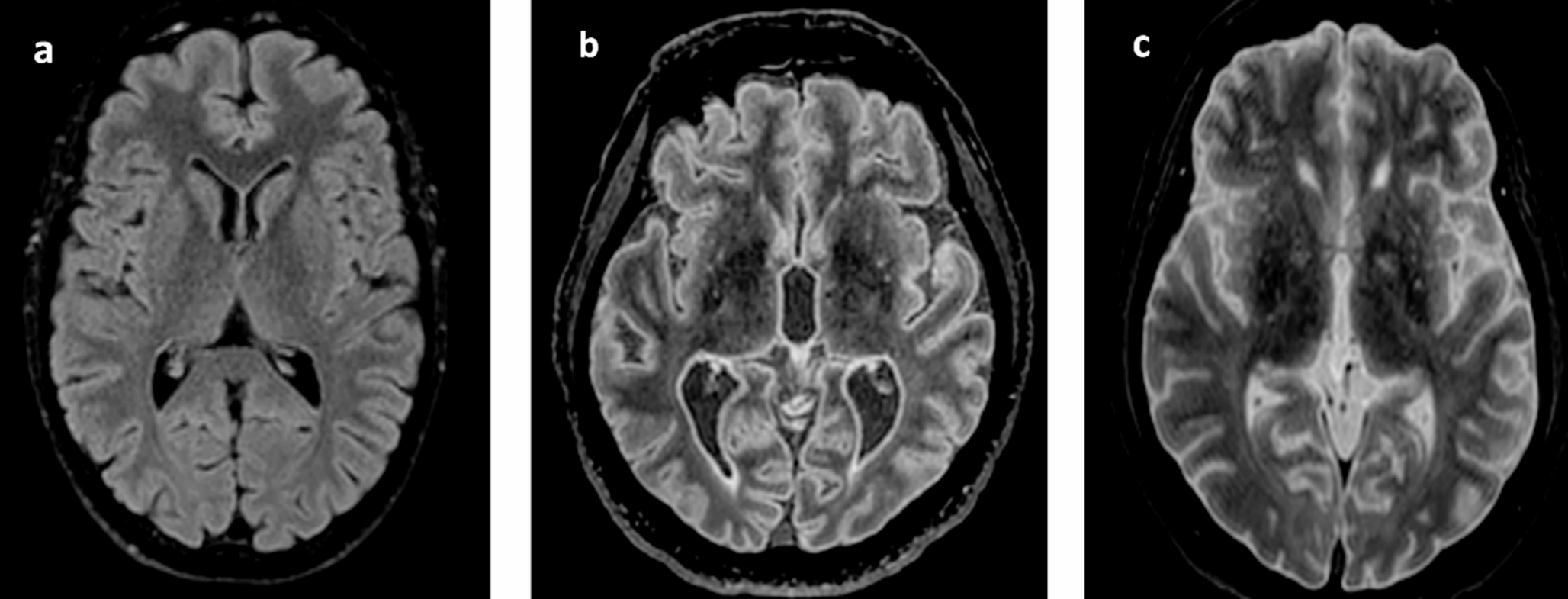
In postmortem imaging, however, the contrast obtained with the 3D FLAIR sequence does not correspond to that of standard clinical 3D FLAIR images, making reliable interpretation difficult. Like other research teams, we have observed substantial contrast variability in this sequence across different postmortem cases. These discrepancies arise even when using the TI values recommended by the manufacturer for clinical use, for instance, 1660 ms on our imaging system (Figs. 1 and 2).
Fig. 1
Axial reconstruction of a 3D sagittal cerebral FLAIR acquisition with a TI at 1660 ms: a) in the living at 36.8 °C; b) a corpse at 29.7 °C (Interval DC-PMMR: ~ 13 h); c) a corpse at 5.7 °C (Interval DC-PMMR: ~ 74 h)
Fig. 2
Axial reconstruction of a 3D sagittal cerebral FLAIR acquisition with a TI at 1660 ms: a) & b) two corpses at 19.5 °C with similar contrast image
We also observed, fortuitously, that cases with similar body temperatures at the time of the MR examination exhibited comparable image contrast (Fig. 2).
According to the literature [5, 6, 21, 22], two variables appear to be primarily responsible for this phenomenon: the body temperature measured immediately prior to the PMMR examination, and the interval between the time of death certification (i.e., the official declaration of death by a physician) and the start of the PMMR scan (DC–PMMR interval).These variables can influence moreover a sequence parameter, the Inversion Time [12, 23,24,25].
Solutions were proposed by some authors to achieve image quality comparable to clinical images. These include, for example, extrapolation methods based on physical models quantifying the MRI signal [12] and the use of TI mapping derived from a 3D VIBE sequence, which differs from the conventional 3D FLAIR sequence [26].
However, we were unable to implement these approaches, primarily due to differences in sequence architecture (e.g., 2D vs. 3D acquisitions or variations in basic sequence parameters), as well as the complexity of certain algorithmic calculations, which proved impractical to perform in real time during PMMR acquisition [27].
Consequently, we opted for an empirical method compatible with the available tools at our disposal. We introduced rapid pre-sequences with empirically adjusted inversion times (TI) at regular, predefined intervals. Although these images were not suitable for diagnostic purposes, they allowed us to optimize image contrast and obtain interpretable results.
We chose this approach despite the availability of advanced tools, such as the “SyntheticMR, Linköping, Sweden”, which enables rapid post-processing reconstruction to generate images with various contrasts by adjusting parameters like TI, TR, and TE. Such tools, as described by some authors [28], can produce “synthetic” FLAIR images; however, we currently do not have access to these resources, as several other forensic institutes.
By adapting the inversion time (TI) using our empirical method, we achieved a significant improvement in the image contrast of the 3D FLAIR sequence. However, the choice of the time for TI modification was influenced by the individual radiographer’s judgment and experience. To ensure consistent diagnostic image quality, it was necessary to address this variability. Given the empirical nature of our approach, we first sought to verify whether our data exhibited similar trends to those reported in previous studies before proposing a reproducible solution.
The aim of this study was to assess whether the relationship between TI in the 3D FLAIR sequence and body temperature observed in our data corresponded to that reported in the literature. Additionally, we evaluated the correlation between TI and the interval from death certification to the start of PMMR (DC–PMMR interval), as described in prior studies.
Comments (0)