
Remember me


A total of 59 patients were enrolled at 20 centers across Japan and evaluated for safety; one patient was not evaluable for effectiveness, so effectiveness was analyzed in 58 patients (see Supplementary results for further information on the effectiveness analysis set). Of all 59 patients, 39 were males (66.1%), 20 were females (33.9%), and the median age was 22 years (< 15 years, n = 22 (37.3%); 15–64 years, n = 36 (61.0%); ≥ 65 years, n = 1 (1.7%) (Table 1).
Table 1 Participant characteristicsPrimary diseases requiring HSCT were hematologic malignancies (n = 22, 37.3%), aplastic anemia (n = 7, 11.9%) and other diseases (n = 30, 50.9%; Table 1). The most common hematologic malignancies were acute myeloid leukemia (n = 7), acute lymphocytic leukemia (n = 6) and myelodysplastic syndrome (n = 3). Of other diseases, the most common were X-linked lymphoproliferative syndrome (n = 8) and chronic active Epstein–Barr virus disease (n = 7) (Table S1).
HLA type mismatches between donor and recipient were reported in 57/59 patients; 11 patients (18.6%) had a match with the donor, seven patients (11.9%) had one locus mismatch and 39 patients (66.1%) had ≥ 2 mismatched loci.
Twenty patients (33.9%) had a medical history of comorbidities, and 28 (47.5%) had complications, including infection (n = 9; 15.3%), liver disease (n = 6; 10.2%), cardiac disease (n = 3; 5.1%) or kidney disease (n = 1; 1.7%).
Alemtuzumab and HSCTPrior to HSCT, 54 patients (91.5%) received conditioning with a drug other than alemtuzumab, 25 (42.4%) received radiation, and one patient (1.7%) received the HLH-94 treatment protocol for hemophagocytic lymphohistiocytosis. The most common conditioning regimens were busulfan plus fludarabine phosphate (n = 15), cyclophosphamide hydrate plus total body irradiation ([TBI]; n = 7), melphalan plus fludarabine phosphate plus TBI (n = 7), busulfan plus melphalan plus fludarabine phosphate (n = 6) and busulfan plus fludarabine phosphate plus TBI (n = 5).
Stem cells for transplantation were sourced from peripheral blood in 36 patients (61.0%), bone marrow in 22 patients (37.3%) and umbilical cord blood in one patient (1.7%). Donors were siblings in 22 cases (37.3%), non-sibling relatives in 21 cases (35.6%) and unrelated individuals in 16 cases (27.1%).
Of the 59 included patients, 37 discontinued treatment during the 6-day treatment period: 30/37 (81.1%) terminated treatment as planned; 1/37 (2.7%) discontinued treatment due to primary disease progression; and 6/37 (16.2%) discontinued for other reasons (Table S2). Overall, the mean ± SD duration of treatment with alemtuzumab was 3.7 (1.1) days. Alemtuzumab was administered consecutively for 2 days in four patients (6.8%), for 3 days in 31 patients (52.5%), for 4 days in six patients (10.2%), for 5 days in 15 patients (25.4%), and for 6 days in two patients (3.4%). One patient (1.7%) received 2 courses of alemtuzumab first for 4 days before HSCT, then after an interval of approximately 40 days for another 3 days before undergoing a second HSCT. The total dosage of alemtuzumab ranged from 0.25 to 1.12 mg/kg (median 0.48 mg/kg; mean ± SD, 0.60 ± 0.19 mg/kg).
All 59 patients received concomitant medications, most commonly consisting of corticosteroids, antivirals, antihistamines, antipyretics, analgesic/anti-inflammatory agents and antibiotics. GVHD prophylaxis consisted mainly of cyclosporine and methotrexate. Alkylating agents were used as concomitant drugs for primary diseases. GVHD was confirmed in four of 58 patients included in the effectiveness analysis; a 46-year-old male (grade 3, onset on day 21, duration of 46 days), a 16-year-old male (grade 3, onset on day 39, duration of 77 days), a 37-year-old male (grade 3, onset on day 31, duration of 50 days) and an 11-year-old male (grade 2, onset on day 21, duration of 56 days).
SafetyOverall, 38 out of 59 patients exposed to alemtuzumab (64.4%) developed an ADR (Table 2). The most common ADRs were fever associated with infusion reactions (n = 22; 37.3%), CMV-related AEs (n = 7, 11.9%), infusion-related reaction (n = 3; 5.1%), adenovirus infection (n = 2; 3.4%), nausea (n = 2; 3.4%), hemorrhagic cystitis (n = 2; 3.4%), decreased lymphocyte count (n = 2; 3.4%) and engraftment failure (n = 2; 3.4%).
Table 2 Adverse drug reactions in the safety analysis set (n = 59): Overall, by organ system class and specific events occurring in ≥ 2 patientsSerious ADRs occurred in 24 patients (40.7%), most commonly CMV-related AEs (n = 7, 11.9%), febrile neutropenia (n = 3; 5.1%) and adenovirus infection, hemorrhagic cystitis and engraftment failure (n = 2 each; 3.4%). One 3-year-old patient died of a serious ADR (multi-organ dysfunction syndrome and pulmonary hemorrhage) 58 days after the end of alemtuzumab treatment, which he received for 4 days as planned.
At the time of database lock, four serious ADRs had not resolved (adenovirus infection, cytokine storm, vascular disorder and multiple organ dysfunction syndrome) and the outcome of one ADR (disseminated intravascular coagulation and thrombotic microangiopathy) was unknown. Apart from these four SAEs and the death reported above, all other serious ADRs were recovered or recovering.
ADRs of grade ≥ 3 occurred in 16 patients (27.1%): febrile neutropenia in three patients (5.1%); adenovirus infection, fever, decreased lymphocyte count, infusion-related reaction and engraftment failure in two patients each (3.4%); bronchopulmonary aspergillosis, CMV chorioretinitis, streptococcal bacteremia, pseudomonas sepsis and human herpesvirus-6 encephalitis, GVHD, hypoxia, hemorrhagic cystitis and hepatic enzymatic abnormalities in one patient each (1.7%).
Infusion reactions occurred in 24 patients per physician reports and in 25 patients (42.37%) per MeDRA/J AE reports. There were no cases of autoimmune hemolytic anemia, autoimmune thrombocytopenia, progressive multifocal leukoencephalopathy, or reactivation of hepatitis B virus.
There were statistically significant differences in the incidence of ADRs according to primary disease and stem cell source, and number of HLA mismatches (Table S3). Fever occurred more frequently in patients with aplastic anemia (5/7; 71.4%) or other primary diseases (13/30; 43.3%) than in those with hematologic malignancies (4/22; 18.2%).
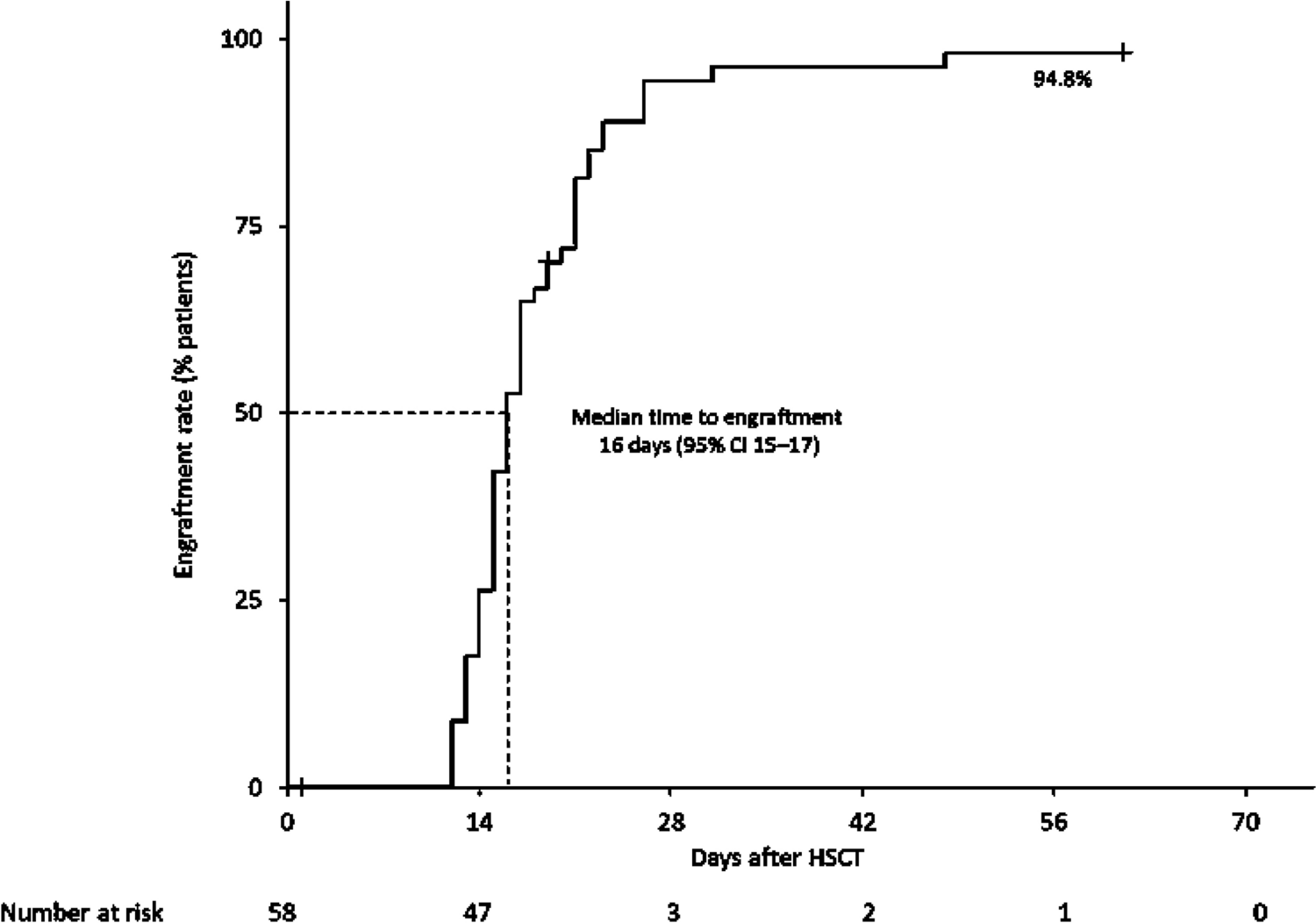
EffectivenessOf 58 patients evaluable for effectiveness, 55 achieved engraftment between 12 and 48 days (median 16; 95% CI 15–17) after HSCT (Fig. 1); therefore, the engraftment rate was 94.8% (95% CI 85.6 to 98.2). Three patients (one child [described earlier] and two adults) died within 60 days of undergoing HSCT, therefore the overall survival rate was 94.8% at day 60. The child (3 years; male) was diagnosed with thrombotic thrombocytopenic purpura and died 49 days after HSCT. An 18-year-old female patient who had posterior reversible encephalopathy syndrome died 28 days after HSCT and a 58-year-old male patient who had acute respiratory distress syndrome died 19 days after HSCT. Although we did not collect information about early death, this possibility cannot be denied. Engraftment was confirmed in all three cases before death. Therefore, these deaths were deemed to not be related to delayed engraftment.
Fig. 1
Kaplan–Meier graph for time to engraftment in the effectiveness analysis set (n = 58). CI confidence interval, HSCT hematopoietic stem cell transplant
Acute GVHD developed in four patients, including grade ≥ 3 acute GVHD in one patient with hematologic malignancies and grade ≥ 2 acute GVHD in three patients with other diseases; therefore, the success rate was 87.9% (n = 51/58; Table 3). The success rate was 90.5% in children aged < 15 years (n = 19/21), 86.5% in adults aged ≥ 15 to 64 years (n = 32/37) and 100.0% in an older patient aged 65 years who met the criteria for success.
Table 3 Treatment response by total dose in the effectiveness analysis set (n = 58)
Comments (0)