
Remember me






Among the 233 participants with mild COVID-19 infection within 1 month (50.6% female, median age 39.4 ± 10.5 years), all individuals completed neuropsychiatric follow-ups at 3 months post-infection (Table 1). Compared with the acute phase, fatigue, anxiety, and depression severity decreased by 3 months, and improvements were observed in executive function and working memory scores. However, recognition function declined, and symptoms of PTSD and sleep disturbances showed no significant improvement at the 3-month follow-up.
Table 1 Demographic characteristics and performance on neuropsychiatric assessments for participants with mild COVID-19 during the acute phase and at 3 months post-infectionNotably, 68.2% and 50.2% of individuals experienced fatigue during the acute phase and 3 months after infection, respectively. The scores on the five dimensions of fatigue decreased over time, but the dominant characteristics were different. During the acute phase, general fatigue, physical fatigue, and reduced activities were the most prominent dimensions. By 3 months post-infection, general fatigue, reduced activities, and mental fatigue became the dominant characteristics.
Cross-sectional univariate analysis of fatigue dimensions and neuropsychiatric symptoms across two post-infection phasesFor Pearson correlation analyses of cross-sectional phenotypes, results showed that all five fatigue dimensions were positively associated with PTSD, anxiety, depression, and sleep disturbances, with the strongest correlation between mental fatigue and depression (r = 0.506, p < 0.001). Additionally, mental fatigue, reduced activity, and reduced motivation were negatively correlated with working memory and executive function, with the strongest correlation between reduced motivation and TMT-B (r = 0.198, p < 0.001) (Supplemental Fig. 1a). A similar pattern was observed at 3 months post-infection. (Supplemental Fig. 1b).
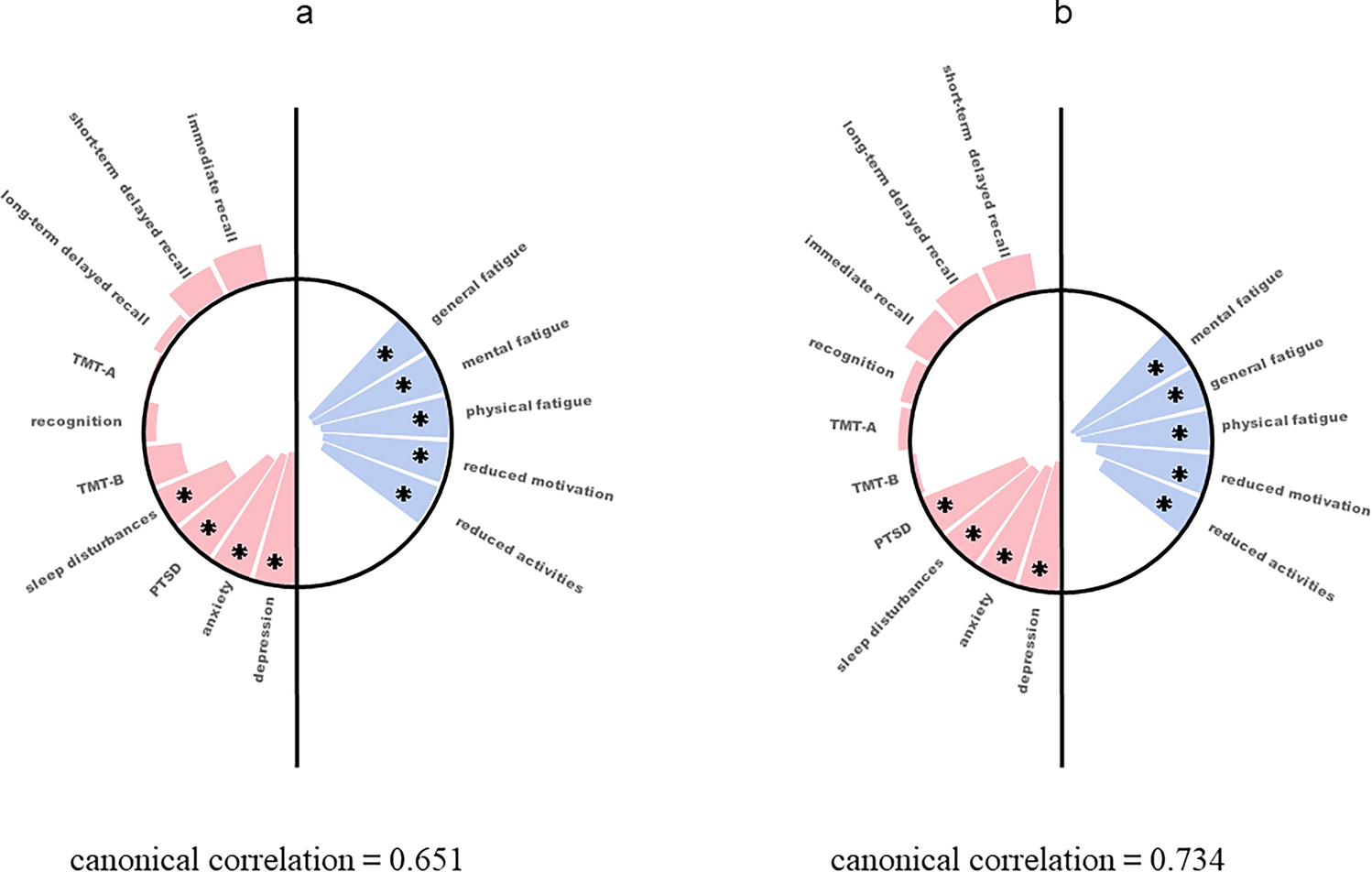
Cross-sectional multivariate analysis of fatigue dimensions and neuropsychiatric symptoms across two post-infection phasesThrough multivariate canonical correlation analysis (CCA), five pairs of canonical variables were extracted for each post-infection phase. The observed cross-sectional univariate associations were effectively captured by the first canonical variate, which explained 95.1% and 95.9% of the shared variance between the five dimensions of fatigue and the ten neuropsychiatric assessments in each phase. The canonical correlation coefficients were r = 0.651 for the acute phase and r = 0.734 for the 3-month post-infection phase, both with p < 0.001.
In the acute phase, fatigue was primarily represented by general fatigue (ρ = − 0.876), mental fatigue (ρ = − 0.875), physical fatigue (ρ = − 0.832), reduced motivation (ρ = − 0.813), and reduced activity (ρ = − 0.796), while the neuropsychiatric component was dominated by depression (ρ = − 0.860), anxiety (ρ = − 0.833), PTSD (ρ = − 0.767), sleep disturbance (ρ = − 0.517), executive function (ρ = − 0.255), and memory measures (ρ = 0.236 for immediate recall, ρ = 0.208 for short-term delayed memory). The strongest associations were between fatigue and depression, anxiety, PTSD, and sleep disturbance. General and mental fatigue were most strongly linked to the exacerbation of these symptoms (Fig. 1a).
Fig. 1
Cross-sectional multivariate analysis of fatigue dimensions and neurological and neuropsychiatric symptoms at two post-infection phases (a: acute phase, b: 3 months post-infection). Bars extending inside the circle indicate negative canonical loadings, while those outside the circle indicate positive canonical loadings. The bar length represents the absolute value of the canonical loadings, and variables with loadings greater than 0.3 are marked with an asterisk (*)
At 3 months post-infection, the fatigue component was again dominated by mental fatigue (ρ = − 0.914), general fatigue (ρ = − 0.895), and physical fatigue (ρ = − 0.870), with reduced motivation (ρ = − 0.762) and reduced activity (ρ = − 0.690) also contributing. The neuropsychiatric component was primarily represented by depression (ρ = − 0.863), anxiety (ρ = − 0.815), sleep disturbance (ρ = − 0.754), PTSD (ρ = − 0.736), and memory measures (ρ = 0.249 for short-term delayed recall, ρ = 0.235 for long-term delayed memory). The joint multivariate association was most strongly influenced by depression, anxiety, sleep disturbance, and PTSD. Mental fatigue showed the strongest correlation with the exacerbation of these symptoms (Fig. 1b).
Performance of neuropsychiatric symptoms across the four longitudinal fatigue trajectory groupsAmong the 159 individuals with acute-phase fatigue, over half reported persistent fatigue at 3 months. In the acute phase, those with persistent fatigue had significantly higher scores in fatigue, PTSD, anxiety, depression, and sleep disturbances compared to those without persistent fatigue. This group also experienced more pronounced physical and mental fatigue. At 3 months, individuals with persistent fatigue showed elevated scores across all fatigue dimensions, along with increased psychiatric symptoms (PTSD, anxiety, depression, and sleep disturbances) and neurological impairments, including deficits in short-term delayed recall and TMT-A performance (Table 2).
Table 2 Performance on neuropsychiatric assessments for participants with persistent fatigue and with alleviated fatigue during the acute phase and at 3 months post-infectionAmong the 74 participants without acute-phase fatigue, 49 remained fatigue-free, while 25 developed new-onset fatigue. In the acute phase, the new-onset group had higher scores for reduced activity and lower immediate and long-term delayed recall compared to the fatigue-free group. At 3 months, they exhibited significantly higher fatigue scores, increased neuropsychiatric symptoms (PTSD, anxiety, depression, and sleep disturbances), and impairments in long-term delayed recall (Table 3).
Table 3 Performance on neuropsychiatric assessments for participants with no fatigue throughout and with the new onset fatigue during the acute phase and at 3 months post-infectionLongitudinal univariate analysis of fatigue dimensions and neuropsychiatric symptoms across the four longitudinal fatigue trajectory groupsFor Pearson correlation analyses of longitudinal phenotypes, persistent fatigue group showed that increases in general, mental, and physical fatigue were mildly associated with changes in anxiety and depression, with the strongest correlation observed between mental fatigue and depression (r = 0.457, p = 0.002). Fatigue dimensions were also slightly associated with declines in working memory and executive function, particularly between general fatigue and short-term delayed recall (r = 0.220, p = 0.022; Supplemental Fig. 2b).
In alleviated fatigue group, increases in all fatigue dimensions were mildly to moderately associated with changes in anxiety, depression, and sleep disturbances, with mental fatigue showing the strongest association with depression (r = 0.316, p < 0.001). No associations were observed with working memory or executive function (Supplemental Fig. 2a).
In no fatigue group, increases in physical fatigue were mildly correlated with changes in depression, while changes in reduced activity and reduced motivation were associated with short-term delayed recall (Supplemental Fig. 3a).
In new-onset fatigue group, increases in reduced activity were moderately associated with declines in executive function (TMT-A), while reduced motivation was correlated with increases in depression (Supplemental Fig. 3b).
Longitudinal multivariate analysis of fatigue dimensions and neuropsychiatric symptoms across the four longitudinal fatigue trajectory groupsThrough the multivariate analysis with CCA, five pairs of canonical variables were extracted from persistent fatigue group. The first pairs of canonical variables showed significant (P = 0.010), and the canonical correlation coefficient were 0.624, which was included in the follow-up analysis. The top of fatigue component was well represented by the change of general fatigue (canonical loadings ρ = − 0.733), mental fatigue (ρ = − 0.677), physical fatigue (ρ = − 0.432), and reduced activity (ρ = 0.420), while the neuropsychiatric component was most represented by anxiety (ρ = − 0.673), depression (ρ = − 0.639), recognition (ρ = 0.351), short-term delayed memory (ρ = 0.305), sleep disturbance (ρ = − 0.299) and executive function (TMT-B, ρ = − 0.262). The multivariate association between changes in fatigue characteristics and neuropsychiatric symptoms over time was strongest for changes in anxiety, followed by depression and memory problems. Longitudinal worsening of general and mental fatigue was associated with worsening of anxiety, depression and memory problems over time (Fig. 2).
Fig. 2
Longitudinal multivariate analysis of fatigue dimensions and neurological and neuropsychiatric symptoms in individuals experiencing persistent fatigue. Bars extending inside the circle indicate negative canonical loadings, while those outside the circle indicate positive canonical loadings. The bar length represents the absolute value of the canonical loadings, and variables with loadings greater than 0.3 are marked with an asterisk (*)
However, no pairs of canonical variables reached statistical significance in the alleviated fatigue group, the no-fatigue group, or the new-onset fatigue group (all p > 0.05).
Comments (0)