Despite advancements in diagnostic modalities, a substantial proportion of HCC cases continue to be diagnosed at an advanced stage, thereby limiting therapeutic options. Since the introduction of sorafenib as the first approved systemic therapy for advanced HCC, the quest for reliable biomarkers to predict treatment response has remained largely inconclusive. This gap underscores the urgent need for prognostic indicators that can guide therapeutic decision-making and support personalized treatment strategies. In this context, the present study investigated the prognostic utility of the pretreatment PNI in patients treated with either sorafenib or regorafenib.
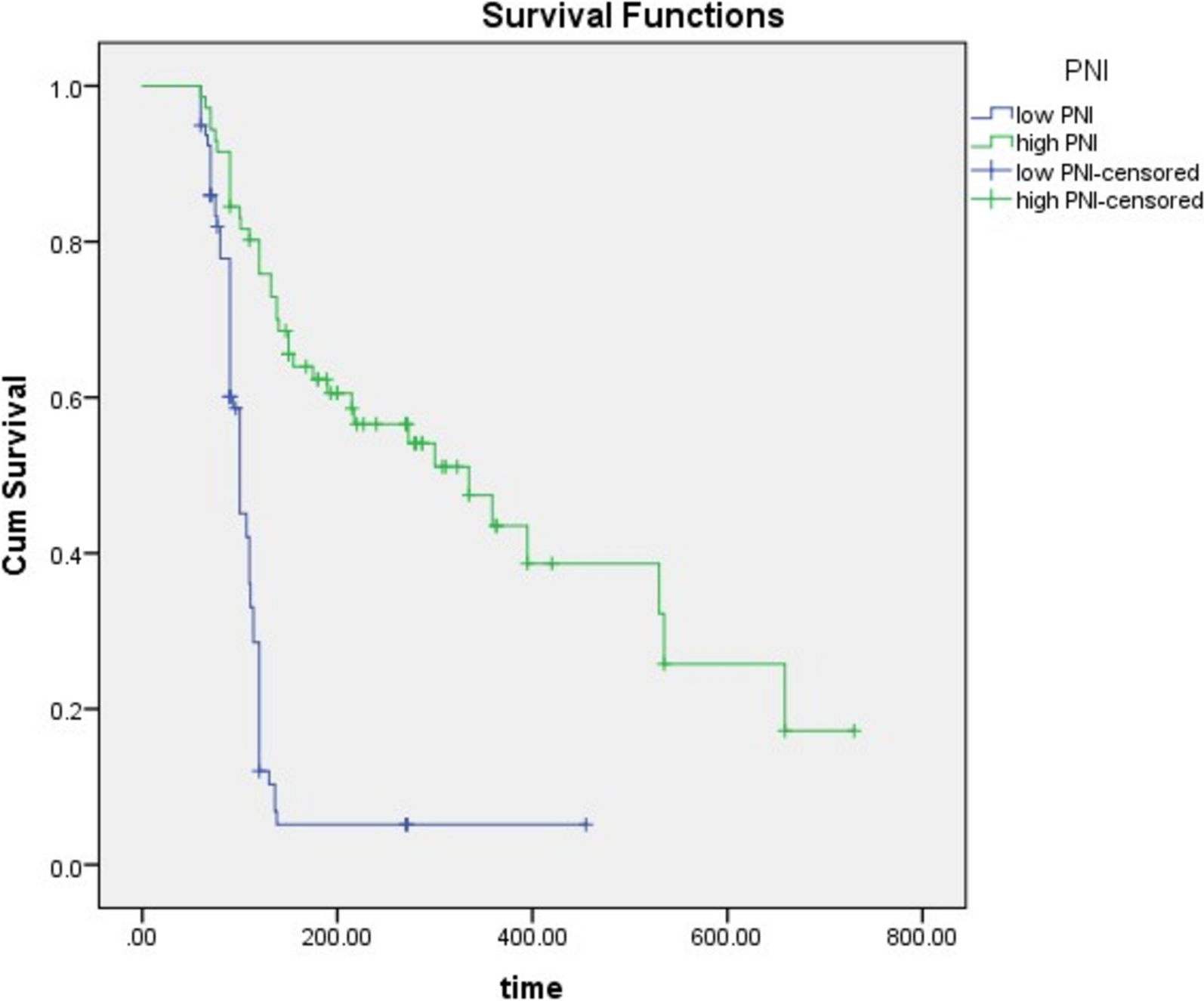
Our results demonstrate that baseline PNI—reflecting both immune and nutritional status—is significantly associated with OS, PFS, and treatment duration in both treatment groups. With a cutoff value of 40.6 (sensitivity: 70%, specificity: 61%), the PNI was a strong prognostic factor, though this threshold differs from prior studies (e.g., Caputo et al.: 31.3; Hatanaka et al.: 46.8) [16, 17]. The PNI, derived from serum albumin and total lymphocyte count, is a simple and accessible index previously validated in various malignancies, including HCC, especially in patients undergoing surgery or transplantation [18, 19].
Our findings are consistent with previous studies, showing that higher PNI predicts improved OS in HCC patients receiving TKIs, including sorafenib and regorafenib [16, 17, 20]. Hiraoka et al. extended these findings to patients on lenvatinib [21]. Our data similarly revealed longer OS in high PNI patients compared to those with low PNI (sorafenib: 6 vs. 3.3 months; regorafenib: 8 vs. 3.7 months), supporting its role as a useful prognostic biomarker.
Additionally, high PNI was associated with prolonged PFS, although no significant differences were observed in objective response rate (ORR) or disease control rate (DCR) across PNI subgroups. These findings align with those of Caputo et al. and Hatanaka et al., who also reported no significant relationship between PNI and ORR or DCR [16, 17]. However, our results contrast with those of Rimini et al., who found no significant PFS difference between PNI groups in patients receiving regorafenib [20].
The mechanisms by which PNI influences survival remain multifactorial. Albumin, a major determinant of PNI, reflects liver synthetic function and systemic inflammation. Hypoalbuminemia is common in cirrhosis and cancer cachexia and has been associated with poor prognosis across cancers, including HCC [22, 23]. Albumin is also a negative acute-phase reactant; its reduction may signal chronic inflammation, malnutrition, and immune suppression. Both albumin and PNI have been advocated as nutritional risk screening tools in oncology [24, 25].
Lymphocytes, the immunological component of PNI, have a pivotal role in anti-tumor immunity. Tumor-infiltrating lymphocytes (TILs) have been linked to favorable outcomes in HCC, as demonstrated by Yao et al., Schoenberg et al., and Unitt et al., who reported associations between TILs and improved OS, PFS, and recurrence-free survival [26,27,28,29]. Our findings support the relevance of lymphocytic status as a prognostic determinant in patients treated with sorafenib, in line with previous research [22].
Beyond PNI, we also identified ALBI grade and Child–Pugh score as important predictors of survival. In the sorafenib group, both scores were associated with better OS and PFS, while in the regorafenib group, ALBI grade alone remained a significant predictor in multivariate analysis. Our results are consistent with those of Diaz-Beveridge et al. and Hatanaka et al., who found that Child–Pugh classification significantly influenced outcomes with sorafenib [17, 30]. However, this contrasts with Presa Ramos et al., who observed no survival differences across Child–Pugh classes [31].
The ALBI grade provides an objective liver function assessment and has demonstrated prognostic value in systemic HCC therapy. Our findings are supported by Nguyen et al. and Xu et al., who reported a correlation between ALBI grade and improved OS in patients treated with sorafenib or regorafenib [32, 33]. Notably, in our regorafenib cohort (90% Child–Pugh A), ALBI grade remained predictive of survival, suggesting its enhanced discriminatory capacity within patients classified as Child–Pugh A. This observation is consistent with Öcal et al., who similarly identified ALBI as an independent predictor in a predominantly Child–Pugh A cohort [34].
Although various inflammation-based indices, such as neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been proposed as prognostic markers in HCC, we found no significant correlation between these markers and survival in multivariate analysis. This finding contrasts with Bruix et al. but aligns with Caputo et al. [16, 35]. The prognostic value of such markers may be confounded by intercurrent conditions (e.g., infections, autoimmune disorders, renal or hematological diseases), underscoring the need for cautious interpretation [36].
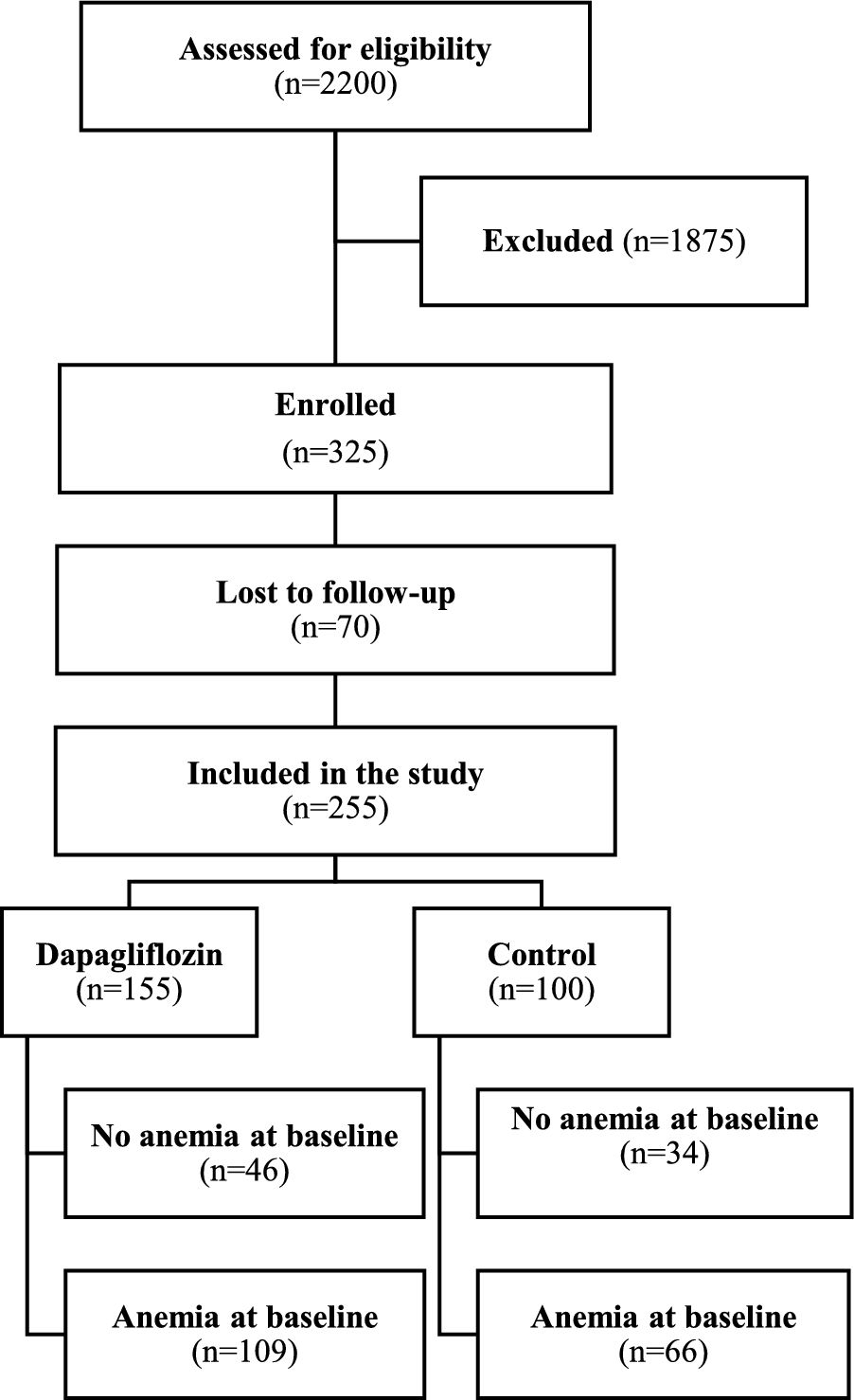
This study has several limitations. First, its retrospective design introduces inherent risks of selection and information bias and limits the ability to establish causality. Second, the exclusion of patients with incomplete data or poor adherence may have affected cohort representativeness. Third, the relatively small number of patients receiving regorafenib (n = 20) limits statistical power and the generalizability of subgroup findings; as such, observed associations between PNI and survival outcomes in this group should be interpreted with caution. Although post hoc power analysis was not feasible due to resource and data constraints, this limitation has been clearly acknowledged.
Moreover, the small sample size in the regorafenib group reflects real-world clinical practice in our setting, where access to second-line treatment is frequently restricted by patient eligibility criteria, including performance status and liver function. These preliminary findings, though limited, offer valuable insights and highlight the need for larger, prospective studies to validate the prognostic role of PNI in second-line therapy. Lastly, the lack of a standardized PNI cutoff across the literature complicates inter-study comparisons and highlights the importance of future efforts toward methodological consistency.




Comments (0)