Setting and participants
The participants were drawn from the SHOT study (Students’ Health and Wellbeing Study), a nationwide survey focusing on students enrolled in higher education across Norway. Since 2010, four major surveys have been conducted, with the most recent wave conducted in 2022. SHOT2022 comprehensively measured various aspects of health and lifestyle, including psychological distress, suicidality, life satisfaction, loneliness, sleep problems, sexual harassment, pain, physical exercise, alcohol and drug use, as well as demographic and educational parameters. Detailed information about SHOT has been published elsewhere [23].
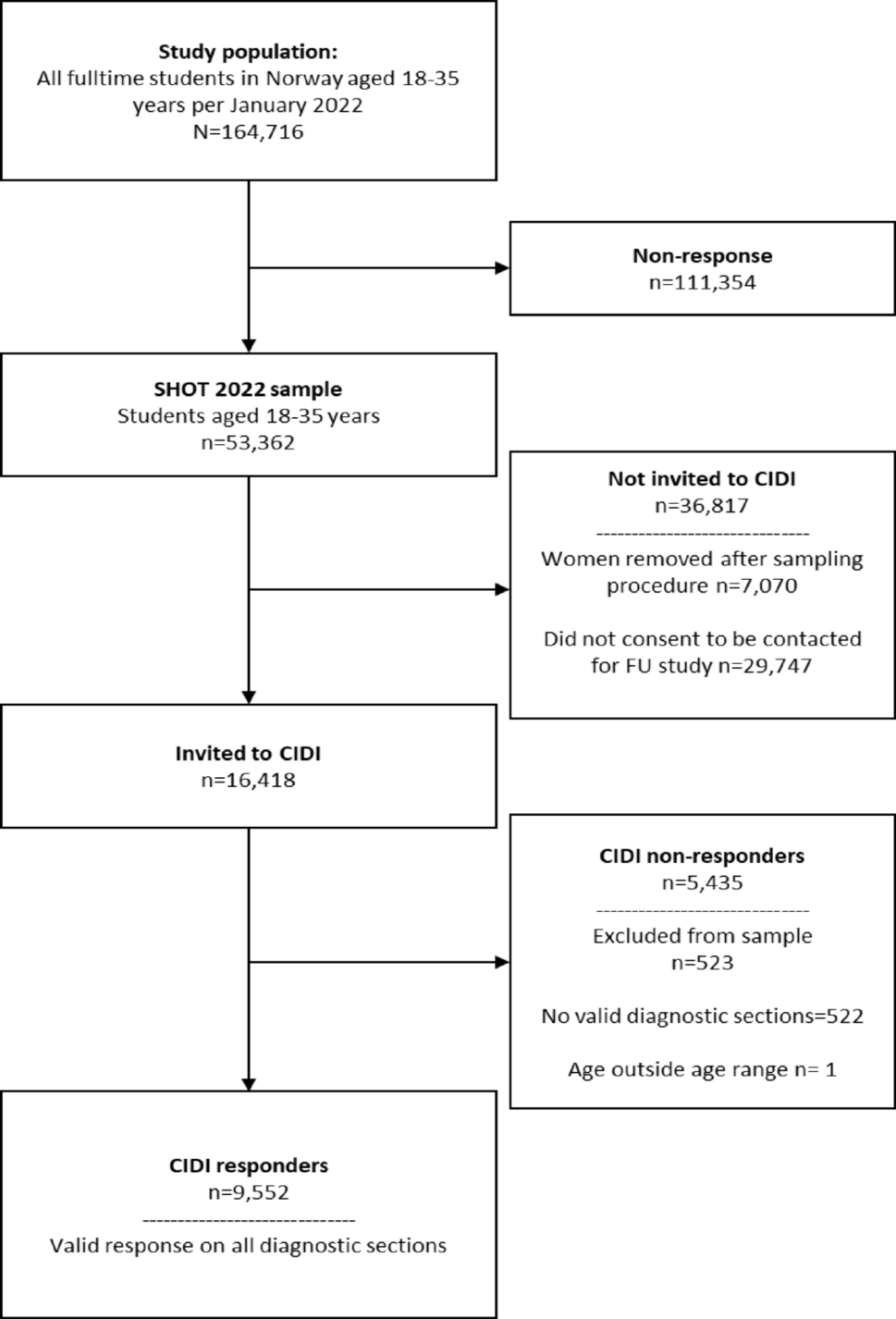
During the survey period, SHOT2022 was distributed electronically through a web-based platform and was open for responses from February 8 to April 19, 2022. All full-time Norwegian students pursuing higher education, both domestically and abroad, were invited to participate. Efforts were made to raise awareness about the study through email, SMS, and information campaigns by numerous welfare organizations and educational institutions. The total number of students was 169,572 (58.4% females), out of which 59,544 students completed the online questionnaires after receiving two reminders. This resulted in a response rate of 35.1%. The response rates across the four health regions in Norway were relatively consistent, ranging from 32.1 to 37.5%, as determined from aggregated data obtained from the Norwegian State Educational Loan Fund. For the current study, a subset of 53,362 students was selected. Inclusion criteria included valid consent for participation in SHOT2022, aged 18–35 years, full-time enrolment in higher education, and completion of key variables relevant to the current analysis (loneliness and CIDI data).
When consenting to participate in the SHOT2022, students were given the option to express their interest in participating in a follow-up study on mental disorders. Out of the total participants, 26,311 students consented to be a part of this follow-up study. To maintain a similar distribution of males and females as in the base study population, a greater number of male students were randomly invited to take part. This resulted in a final invited sample of 16,418 students who were officially registered as students in January 2023. However, the number of male students who consented to being contacted for the follow-up study was relatively lower than females, leading to a higher proportion (70.4%) of females receiving invitations to participate in the CIDI study.
A total of 10,460 students provided valid responses on at least one of the CIDI diagnostic sections, resulting in a conditional response rate of 63.7%. The CIDI study took place between January 24 and February 6, 2023, approximately 12 months after the SHOT2022 survey was conducted. More detailed information on the participation process has been published elsewhere [24]. Fig. 1 details the participation process.
InstrumentsSociodemographic information
Participants’ age and sex information was derived from their 11-digit Norwegian national identity numbers. To gather additional background information, the CIDI study was linked with the SHOT2022 study. In SHOT2022, participants were asked about their relationship status, with response options including ‘single,’ ‘boy-/girlfriend,’ ‘cohabitant,’ ‘married,’ or ‘registered partner.’ Participants were also asked about their or their parents’ birthplace, to determine if either the student or their parents were born outside Norway.
Loneliness
Loneliness was assessed using an abbreviated version of the widely used UCLA Loneliness Scale, known as the “Three-Item Loneliness Scale (T-ILS)” (Hughes et al., 2004). The T-ILS items (lack of companionship, feeling left out, and isolation) were each rated on a 5-point scale (“never”, “seldom”, “sometimes”, “often”, and “very often”). The T-ILS has displayed satisfactory reliability and both concurrent and discriminant validity (Hughes et al., 2004). Both the individual T-ILS items, as well as a total sum score was used in the current study, the latter was categorized into quintiles. For interaction analyses, the total score was dichotomized at the 80th percentile to identify those with high levels of loneliness. More information about loneliness in the SHOT study has been published elsewhere (Hysing et al., 2020). In addition, SHOT2022 also included a single item assessing to what extent the student felt s/he had enough friends at their place of study, with the response options “I have many friends”, “I have some friends”, “I have few friends”, and “I have no friends”.
Mental health problems
Baseline mental health problems in 2022 were assessed using the Hopkins Symptoms Checklist (HSCL-25), a widely used screening tool designed to detect symptoms of anxiety and depression. The HSCL-25 includes a 10-item subscale for anxiety and a 15-item subscale for depression, with each item scored on a 4-point scale ranging from “not at all” [1] to “extremely” [4]. The reference period for the items is the prior two weeks. A prior investigation of the HSCL-25’s factor structure, based on the SHOT2014 dataset, further established that a unidimensional structure, rather than separate subscales for anxiety and depression, exhibits optimal psychometric properties for application to student populations [25]. In this study, we applied sex-specific cutoffs of 1.96 for males and 2.20 for females, as determined in a recent analysis of the SHOT dataset [26]. These updated thresholds were validated against a self-administered version of the Composite International Diagnostic Interview (CIDI). The validation demonstrated that these cutoffs provide an optimal balance between sensitivity and specificity, enhancing the diagnostic precision of the HSCL-25 for use in student populations. To identify individuals with high levels of mental health problems, we dichotomized the HSCL-25 scores based on these cutoffs. Participants scoring above the sex-specific thresholds were categorized as “high scorers,” representing those at elevated risk for significant symptoms of anxiety and/or depression.
Mental disorders: the CIDI
A newly developed self-administered electronic version of the Composite International Diagnostic Interview (CIDI), created for the WHO World Mental Health (WMH) Surveys [27] was used for the data-collection [28]. A detailed description of the development of this self-administered version CIDI version has been published elsewhere [24]. In short, CIDI 5.0 is a standardized interview assessing 30-days, 12 months and lifetime prevalence for several mental and substance use disorders according to diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5) [29]. CIDI 5.0. has good concordance with diagnostic instruments such as the Structured Clinical Interview for DSM-IV (SCID) [30] and Schedules for Clinical Assessment in Neuropsychiatry (SCAN) [31]. The Norwegian version of the CIDI is based on the official Norwegian translation of CIDI 5.0, as described in a previous study protocol publication [32].
A current disorder was defined as the presence of MDE during the 30 days before study. We also calculated the 12-month and lifetime prevalence of MDE, and participants fulfilling either of these criteria, but not current mental disorder (n = 2,789), were omitted from the statistical analyses, given the presents study’s focus on mental disorders being present after the SHOT2022 data collection. The operationalization of MDE was based on algorithms developed for CIDI 5.0 in the WMH Surveys Initiative.
Statistical analyses
All analyses were conducted using unweighted data, as the estimates were presented separately for male and female students, and the age and sex distribution of the sample did not differ, or only marginally differed, from that of the base student population. Descriptive and clinical characteristics (age, sex, marital status, country of birth, and loneliness) were calculated for CIDI responders, non-responders, and the total SHOT2022 sample. Statistical comparisons between CIDI responders and non-responders were performed using Chi-squared tests for categorical variables and independent samples t-tests for continuous variables. The prevalence estimates of major depressive episodes (MDE), stratified by levels of loneliness, were subsequently calculated. Poisson regression models with a log link function and robust standard errors were used to calculate effect sizes for dichotomous variables. Results are presented as risk ratios (RR) with 95% confidence intervals, derived from exponentiated coefficients, adjusting for potential confounders. Model 1 adjusted for age, while Model 2 additionally accounted for symptoms of anxiety and depression, as indicated by high scores on the HSCL-25. To assess potential effect modification by sex, we conducted formal interaction analyses on both the multiplicative and additive scales. For the multiplicative interaction, an interaction term (sex × high loneliness) was included in Poisson regression models, adjusting for age and baseline symptoms of anxiety and depression. Additive interaction was evaluated using standard epidemiological measures: the Relative Excess Risk due to Interaction (RERI), the Attributable Proportion due to interaction (AP), and the Synergy Index (S). These were calculated based on risk ratios derived from a four-level combination variable reflecting sex (male/female) and loneliness (high/low, dichotomized at the 80th percentile of the T-ILS score). Evidence of additive interaction is typically indicated by RERI > 0, AP > 0, and S > 1. All analyses were performed using IBM SPSS version 29.


Comments (0)