
Remember me

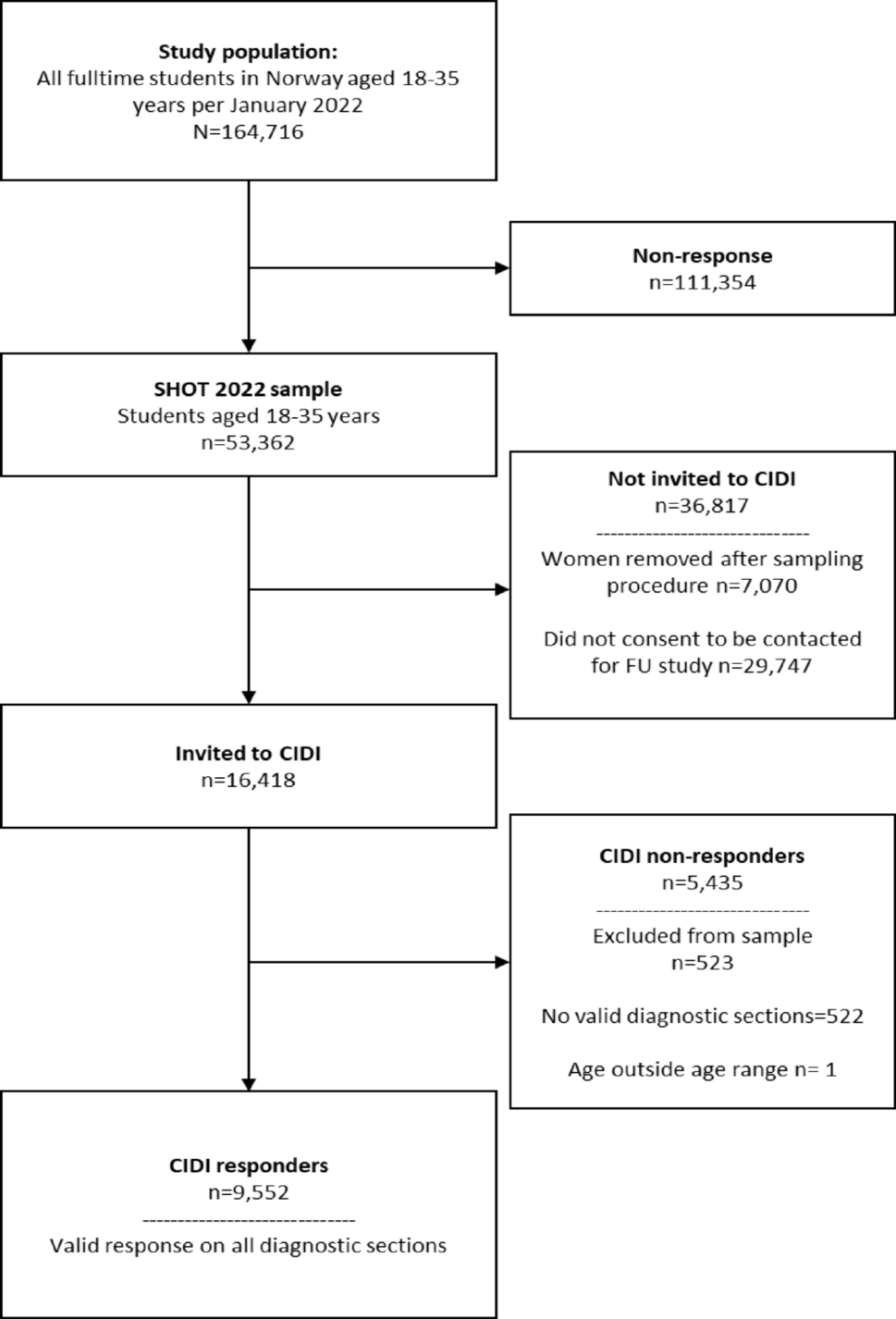
The data in this study was collected as a part of the Africa Focus on Intervention Research for Mental Health – South Africa (AFFIRM-SA) trial, an individually randomised controlled trial aimed at improving maternal depression outcomes among perinatal women in South Africa using a task sharing approach [23, 24]. Data was collected from Khayelitsha, a peri-urban settlement outside Cape Town. There is one district hospital, five community health centres and eight day clinics that serve the population of approximately 400,000 people. Families in this area face high levels of poverty and unemployment. Housing is also in poor condition, often without electricity and water. Residents also tend to live in overcrowded accommodation with poor sanitation systems [23]. Recruitment was carried out at two antenatal clinics that were part of community health centres. Details regarding recruitment and data collection strategies have been described previously [23].
ParticipantsThis analysis uses data from the control arm of the AFFIRM-SA trial (n = 216). The eligibility criteria for the trial were that women had to be at least 18 years of age and no more than 28 weeks pregnant, able to give informed consent and speak isiXhosa, living in Khayelitsha, attending their first antenatal visit, and scoring 13 or higher on the Edinburgh Postnatal Depression Scale (EPDS). Those who required urgent medical or mental health care were excluded. Data were collected from women presenting to two antenatal clinics - Michael Mapongwana Community Health Centre (CHC) or Site B CHC - for routine antenatal check-ups. Eligible participants were randomly assigned to either the control or intervention condition.
MeasuresAll measures used in this analysis were collected at three assessment visits: the first antenatal check-up which was considered baseline; eight months gestation in the antenatal period; and three months postnatal.
ExposureWhen large percentages of a population are poor, typical measures of poverty such as income and consumption alone are not reliable [25]. This is potentially because poorer communities tend to have strong informal networks for sharing resources in cases of scarcity. In addition to this, income and consumption measures are often unreliable in an informal economy [25]. In such instances, a measure such as food insecurity would be more appropriate. We therefore selected food insecurity as our exposure of interest, captured using The Household Food Insecurity Access Scale (HFIAS) [26].
HFIAS captures levels of food insecurity through a questionnaire with answers ranging from 0 (never) to 3 (often) [26, 27]. This results in scores ranging between 0 and 27, with higher scores indicating increasing levels of insecurity. Scores are categorised into the following four levels: (1) Food Secure; (2) Mildly Food Insecure; (3) Moderately Food Insecure, and; (4) Severely Food Insecure [26, 27]. These levels were determined depending on affirmative responses to more severe conditions such as going to bed hungry or going a whole day without eating, and how often these conditions are experienced [27]. For the purposes of this study household HFIAS scores were converted into a binary variable, with households facing either no or mild food insecurity (unexposed), and households facing moderate to severe food insecurity (exposed).
OutcomeOur outcome was symptoms of perinatal depression reducing by at least 40% captured three months after delivery using the Hamilton Depression Rating Scale (HDRS-17) that had been adapted and validated for the AFFIRM trial [28]. The HDRS-17 consists of 17 items ranging from weight loss, insomnia, and agitation to the ability to carry out usual activities [28, 29].
MediatorsA mediator is defined as a variable that is on the causal pathway between the initial exposure (in our case, food insecurity) and the outcome (symptoms of postnatal depression at three months after delivery). It is therefore a variable that is causally influenced by the intervention and in turn causally influences the outcome [30]. Although our mediator of interest is levels of social support, it is also important to capture the mediating effect of other factors associated with food insecurity, levels of social support, and symptoms of postnatal depression. Failing to do so will bias the estimates from our models. Additional mediators were therefore selected if they were associated with levels social support, food insecurity, or symptoms of postnatal depression (p < 0.1). This relatively large p value was selected to ensure that all potential mediators were included to minimise the chances of severe confounding bias in the model.
The mediators for our analyses were captured at the eight-month antenatal visit, prior to the three-month postnatal follow-up visit where the outcome measure was assessed. This helps to rule out reverse causation between mediators and the outcome where there was a sufficient time lag between when the mediators were collected and the outcome of interest.
Based on these criteria, the following mediators were selected:
Number of antenatal visits (Mediator 1(M1))As part of a participant’s antenatal care package, she was offered and attended scheduled antenatal care visits. We anticipated the possibility that food insecurity would influence the number of antenatal visits as those who are highly food insecure would be less likely to spend time and resources attending the health centres. We anticipated attendance to antenatal care visits could influence not only perinatal depression, but also other mediators. This would be because during antenatal visits the health of the mother and baby would be checked, information for a healthy pregnancy and delivery would be provided, leading to women feeling supported and reassured. Potentially this could lead to a reduction in symptoms of depression. To capture this effect, we created a mediator to reflect the number of antenatal sessions attended (n = 1–15).
Suicidality (M2)We theorised that food insecurity could increase the risk of suicidal behaviours [31]. Food insecurity has previously been associated with suicidal behaviours ranging from suicidal ideation to attempts, with theories suggesting that the association is caused due to chronic stress, that it is caused by affecting social supports, and that it caused by exacerbating feelings of hopelessness and fatalism [31]. To capture the effect of food insecurity on suicidality, we used the Suicidality Module of Mini International Neuropsychiatric Interview 6.0.0 captured at eight months gestation [32]. The measure is continuous, with items having different scores, and with higher scores indicating higher levels of suicidality [32].
Social support (M3)Our main hypothesis theorised that increased food insecurity may lead to a reduction in perceived social support that would increase the symptoms of postnatal depression. To capture this effect, we used the Multidimensional Scale of Perceived Social Support (MSPSS), administered at eight months gestation [33]. The MSPSS is a questionnaire with 12 items with answers ranging from Very strongly disagree (1) to Very strongly agree (7). It examines an individual’s perception of the social support they receive from friends, family, and a special person. Scores range from 0 to 84, with higher scores denoting higher levels of social support [33]. The MSPSS has shown to have good reliability (Cronbach’s Alpha: 0.85), and has demonstrated construct validity [33].
Dependency of mediators on one anotherA by-product of the interventional indirect effects is that in addition to the mediator-specific indirect effects, there is another indirect effect via the mediators’ mutual dependence on one another [22]. This indirect effect is close to zero when mediators are conditionally independent and non-zero when mediators interact or covary in their effects on the outcome.
Mediator-outcome confoundersMediator-outcome confounders can generate spurious correlations between the mediator and outcome when unadjusted for, potentially distorting these associations. We considered potential baseline characteristics that are associated with the exposure, mediators, or the outcome, as potential confounders (p < 0.10). The selection process for these confounders is described in the supplementary material.
Statistical methodsGeneralTo better understand how food insecurity influenced the mediators to improve symptoms of postnatal depression, we present (1) unadjusted associations between the selected mediators and food insecurity, and (2) unadjusted associations between selected mediators and symptoms of postnatal depression. This can be seen in Tables 1 and 2 respectively.
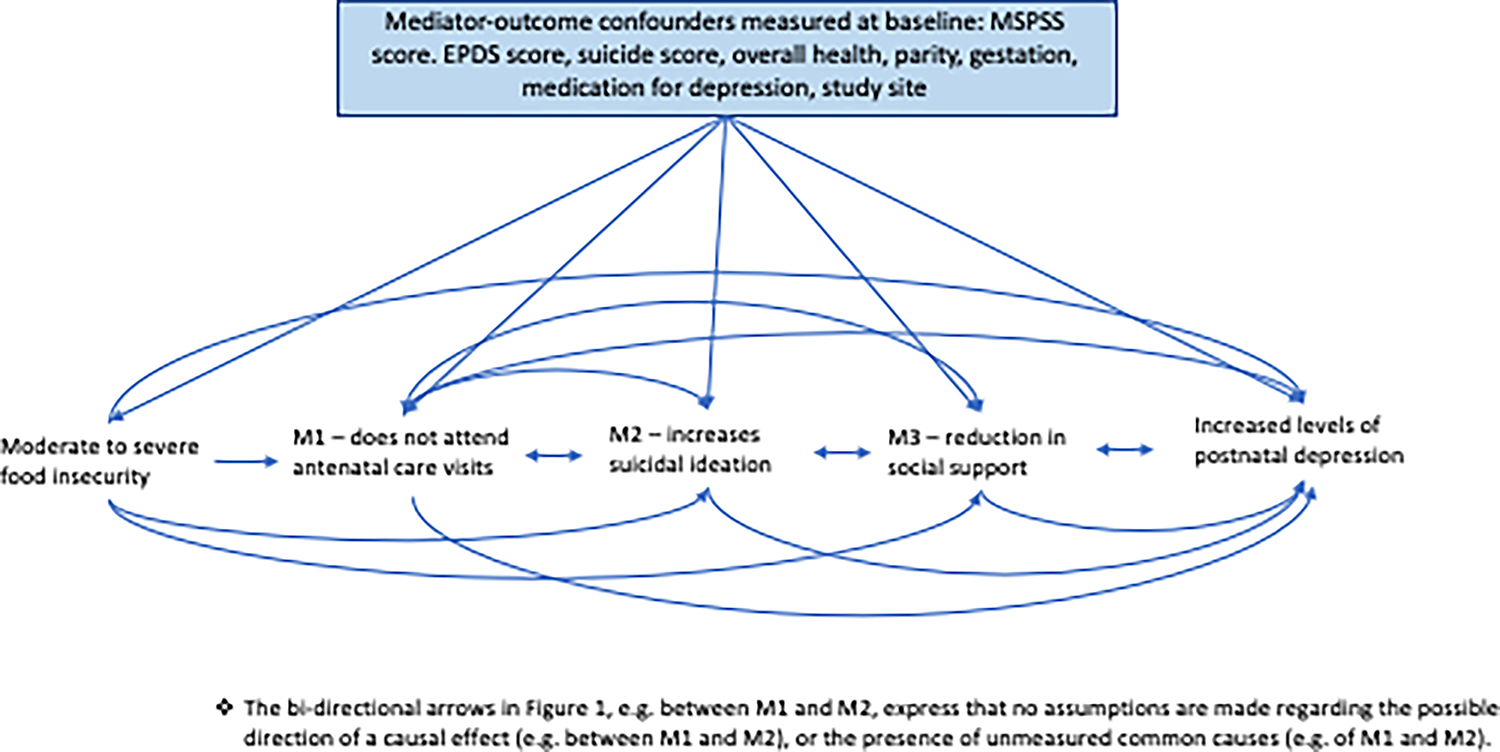
Mediation analysisWe aimed to investigate the extent to which reduced symptoms of perinatal depression captured at three months using the HDRS questionnaire (HDRS scores improved by at least 40% between baseline and three months postnatal) were explained by the indirect effects of number of antenatal visits, suicidality levels, and levels of social support (Fig. 1). To achieve these objectives, we used the interventional (in)direct effects approach to mediation analysis to understand population-level effects relevant to this analysis [22]. Interventional effects are the latest in a series of developments that use an advanced causal inference framework to overcome limitations of other approaches to mediation such as Structural Equation Modelling [34, 35]. Findings for this analyses are described according to guidelines for reporting mediation analyses (AGReMA statement) [30]. Further details on the mediation analysis relating to the interventional effects can be found in the Supplementary Material.
Fig. 1
Causal model demonstrating the proposed pathways through which the exposure to moderate/severe food insecurity may lead to postnatal depression
Estimation and model fitEstimation for the interventional indirect effects was based on Monte Carlo integration using a 1,000-fold expanded dataset [22]. The expanded dataset was created in five steps. Details of each step, and details of the models including interactions and selected confounders can be found in Supplementary Material. Bias-corrected confidence intervals were based on nonparametric bootstrap with 1,000 resamples [22].
AssumptionsThe interventional effects have important underlying assumptions that will influence the validity of our findings if violated. The main assumptions relevant to our study is that there are no unmeasured confounders between the exposure and the mediator, and between the mediator and the outcome.
Sensitivity analysisPrimary outcomes for perinatal depression are reported using different instruments. We selected our outcome based on the primary outcome from the AFFIRM trial. Given different instruments capture different characteristics of perinatal depression, we also conducted the same analyses using outcomes from the Edinburgh Postnatal Depression Score. Specifically, we compared indirect effects using the outcome of HDRS scores reducing by at least 40% between baseline and three months, to that of EPDS reducing by the same percentage [36].
Missing dataTo account for missing data, we implemented single stochastic imputation using chained equations with 10 burn-in iterations, under the assumption that data were ‘missing at random’ (MAR). Imputation models included all mediators, outcome of postnatal depression, and confounders in models to assess interventional effects. Missing variables were imputed separately for exposed (moderate to severe food insecurity) and unexposed participants (none or mild food insecurity. In each of the 1000 bootstrap samples, the imputation is done once.
Comments (0)