Study design
This retrospective, two-center observational cohort study was conducted to evaluate the clinical impact of a specific intraoperative maneuver, hereafter referred to as "Technique R," in patients undergoing minimally invasive surgery for primary colorectal cancer. Eligible patients underwent laparoscopic or robot-assisted colectomy or proctectomy, including ileocecal resection (ICR), right hemicolectomy (RHC), transverse colectomy (T), left hemicolectomy (LHC), sigmoidectomy (S), high anterior resection (HAR), low anterior resection (LAR), abdominoperineal resection (APR), Hartmann’s procedure, and intersphincteric resection (ISR). Patients who required total colectomy for colitic cancer or had multiple synchronous colorectal lesions were excluded.
A total of 1421 consecutive patients who underwent surgery for colorectal cancer between January 2015 and March 2024 at the Osaka International Cancer Institute (formerly Osaka Keisatsu Hospital) and Osaka University were retrospectively reviewed. After excluding 70 patients who were initially scheduled to undergo open surgery, 1351 patients were included in the final analysis. The study protocol was approved by the Institutional Review Boards of both institutions (approval numbers: 1374 and 20163–3). Written informed consent for surgical treatment and the use of clinical data was obtained from all patients prior to enrollment.
Data source and study population
All data were obtained from the hospital’s electronic medical records and cross-validated using operative and pathology reports. Emergency surgeries were not included. Baseline demographic and clinical data collected included age, sex, body mass index (BMI), ASA physical status, comorbidities, prior abdominal surgery, tumor location, use of preoperative chemotherapy, type of surgery, surgical approach (single-port vs. multiport), stoma formation, prognostic nutritional index (PNI) [17], and pathological TNM stage (UICC 8th edition). There were no missing values in the collected variables.
Perioperative management and surgical procedures
All patients were diagnosed preoperatively by colonoscopy with biopsy. Tumor location was defined as the distance from the tumor’s distal edge to the anal verge, based on digital rectal and endoscopic examination. Clinical staging was performed using chest and abdominal computed tomography (CT). Neoadjuvant chemotherapy was selectively offered to patients with clinically staged T3 or T4 tumors or node-positive (N1/N2) non-metastatic disease.
Standard oncologic resections were performed according to the principles of total mesorectal excision (TME) for rectal cancer and complete mesocolic excision (CME) for colon cancer [3, 18], in accordance with the guidelines of the Japanese Society for Cancer of the Colon and Rectum. A diverting stoma was created at the surgeon’s discretion in cases of LAR or ISR. For APR and Hartmann’s procedures, permanent stomas were constructed via the intraperitoneal or retroperitoneal route. Operative time was defined from skin incision to skin closure. Conversion to open surgery was defined as any unplanned incision exceeding 7 cm or deviation from the predetermined incision site.
Postoperative complications and mortality were recorded if they occurred during the same hospital admission or within 30 days postoperatively. Complications were categorized using the Clavien–Dindo classification. Adhesion severity was assessed intraoperatively based on the Zühlke classification, which grades adhesions from 0 (none) to 4 (very dense, with high risk of organ injury) [19].
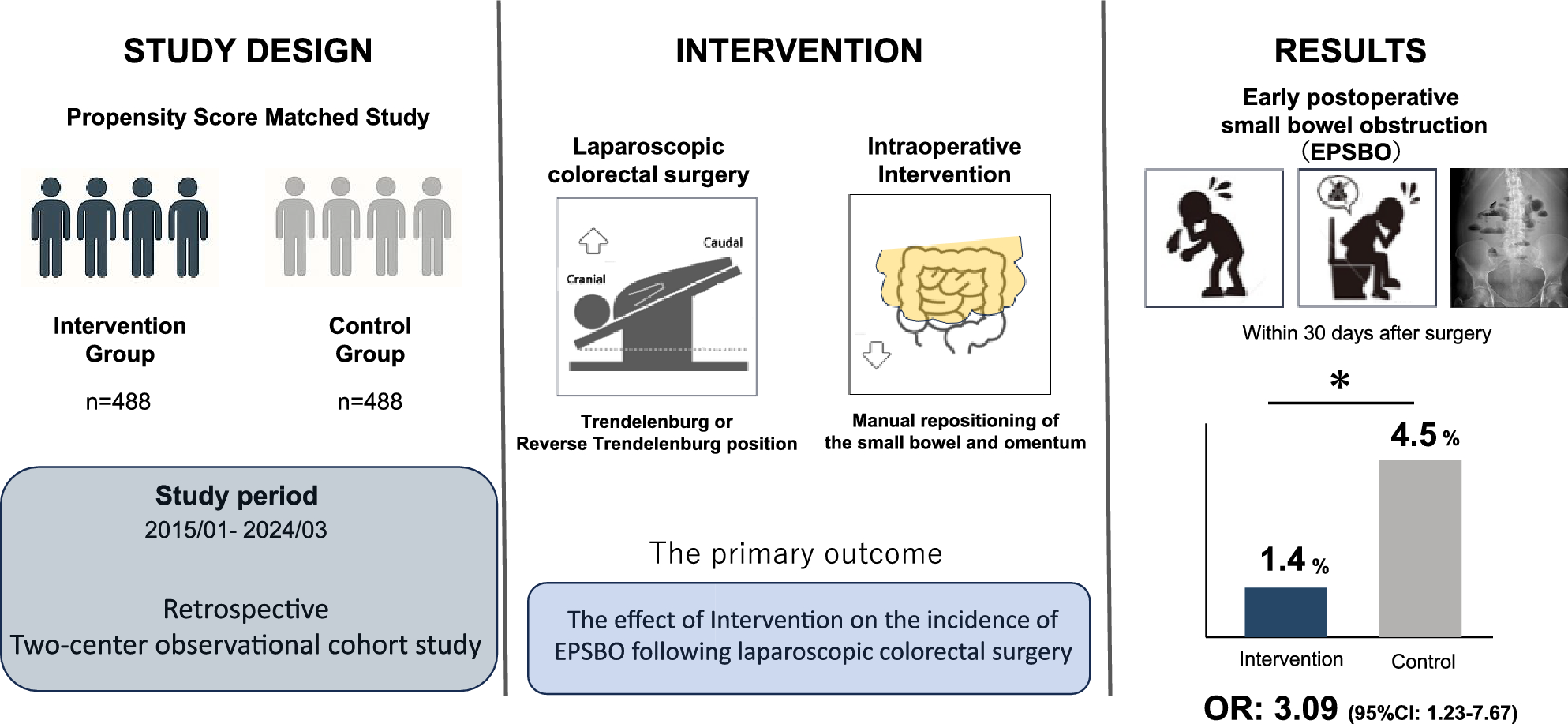
Throughout all procedures, the small intestine and omentum were displaced from the surgical field using gravity in the Trendelenburg or reverse Trendelenburg position. Technique R was defined as the manual repositioning of the small intestine and omentum to their anatomical locations after restoration of the neutral position and completion of all surgical steps. In all cases, after completion of the surgical procedure, the patient’s position was returned from the operative position (typically Trendelenburg with lateral tilt) to the horizontal position. Subsequently, the small intestinal mesentery was manually and carefully realigned to its original anatomical orientation, with particular attention to avoid unnatural twisting or folding. Finally, the greater omentum was gently spread over the small intestine to restore the preoperative intra-abdominal configuration as closely as possible. This procedure was applied uniformly across right hemicolectomy, left hemicolectomy, and low anterior resection. Although the intraoperative positioning differed depending on the type of surgery (Trendelenburg with left tilt for right hemicolectomy, and with right tilt for left hemicolectomy), the final step of returning the patient to the horizontal position and manually restoring the intra-abdominal anatomy remained the same. This maneuver was not employed before 2019 (Group A) but was consistently applied thereafter (Group B). In addition, the mesenteric defect created during right hemicolectomy was not routinely closed; it was left open in all cases. For all right-sided resections, extracorporeal functional end-to-end anastomosis was consistently performed, and the orientation was uniformly isoperistaltic. The use or omission of manual repositioning (Technique R) was clearly documented in all operative reports, and we reviewed the operative notes of all cases to verify its implementation status.
A total of eight colorectal surgeons participated in this study. The adoption of Technique R was implemented in a structured, department-wide manner in 2019, following the appointment of a new chief surgeon. All participating surgeons were certified specialists in gastrointestinal and colorectal surgery and had completed endoscopic surgical certification. Although some staff rotations occurred during the study period, the technical implementation of Technique R was standardized across the department after its formal introduction.
Outcome measures
The primary outcome was the effect of Technique R on the incidence of early postoperative small bowel obstruction (EPSBO) following minimally invasive colorectal surgery. EPSBO was defined as the presence of clinical symptoms such as abdominal distension, nausea, or vomiting within 30 days postoperatively, along with no passage of stool for over 24 h, and radiological confirmation of dilated bowel loops with multiple air-fluid levels on plain abdominal X-ray or CT scan. While nasogastric tube reinsertion was performed when clinically necessary, it was not used as a diagnostic criterion. In this study, mechanical SBOs and paralytic ileus were not differentiated, as both conditions contribute similarly to early postoperative obstruction in the clinical context. The secondary objective was to identify potential risk factors associated with EPSBO.
Statistical analysis
Continuous variables were reported as medians with interquartile ranges (IQR), and categorical variables as frequencies and percentages. Pre-matching comparisons were performed using Student’s t-test or Wilcoxon rank-sum test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. A two-tailed p-value < 0.05 was considered statistically significant.
To reduce selection bias and adjust for confounding, propensity score matching (PSM) was performed using a 1:1 nearest-neighbor algorithm with a caliper width of 0.2. Propensity scores were derived from a multivariate logistic regression model that included the following 10 covariates considered relevant to surgical complexity: sex, age, BMI, ASA classification, history of abdominal surgery, TNM stage, tumor location (left-sided vs. right-sided), prognostic nutritional index (PNI), precise tumor location, and surgical approach (single-port vs. multiport).
Matched pairs were used to compare the incidence of EPSBO between Group A and Group B. Baseline covariates, including those not used for matching, were assessed using bivariate analysis.
The univariate and multivariate logistic regression analyses were conducted to identify independent predictors of postoperative EPSBO. All statistical analyses were conducted using JMP Pro version 17.0.0 for Mac (SAS Institute Inc., Cary, NC, USA).
Univariate analysis was performed to evaluate the crude association between each variable and the occurrence of EPSBO without adjusting for other covariates. Variables with p < 0.05 in univariate analysis were subsequently entered into a multivariate logistic regression model, which allowed adjustment for multiple covariates simultaneously to determine the independent effect of each factor.





Comments (0)