Participant surgeons
A prospective, exploratory, observational cohort study was conducted. The local Ethics Committee was consulted before the start of the study and stated that no specific ethical approval was required. Two experienced pancreatic surgeons from the General and Pancreatic Surgery Unit of the Integrated University Hospital of Verona, a high-volume center for minimally invasive pancreatic surgery, were enrolled (AE, LL), both with extensive expertise in laparoscopic and robot-assisted DP. Both surgeons were male, right-handed, and aged 47 years old. Each had completed the learning curve for both laparoscopic and robot-assisted DP. The years of surgical practice following residency completion were 15 years. The individual caseload of overall pancreatic procedures, including open procedures, exceeded 1000 cases, while the average number of annual open and minimally invasive DP was 40 and 90, respectively. Both underwent a detailed baseline assessment as described below. The surgeons performed 10 procedures as the first surgeon and 10 as the first assistant at the bedside, changing the role, respectively.
Stabilometry and postural stability
Surgeons did not receive ergonomic training and were advised to avoid additional physical activity to prevent muscle injuries. Surgeons’ balance and adjustments were assessed using the Lizard Ultimate stabilometric platform (Lizardmed Srl, Monza, Italy), which monitors center of gravity movements. Standardized tests measured the contributions of vestibular, visual, proprioceptive, occlusal, and cervical systems to posture, with loads expressed in kilograms (kg) and percentages (%). Performance was also evaluated with the Wiva Science device (Letsense, Castel Maggiore, Bologna, Italy). This 3-axis accelerometer measures acceleration along three axes, determining the device’s orientation in space for 3D analysis. Equipped with a gyroscope, it tracks all accelerations and decelerations during movement. By calculating the angular range of primary and secondary movements (ROM), it assesses muscle interference and workload-related fatigue. A pre-study physiatric exam screened for recent muscle injuries or physical issues, such as carpal tunnel syndrome or neck/back disorders. All measurements were taken before and after surgery. Additionally, surgeons were asked to repeat the measurements with eyes open and closed to better evaluate postural stability following surgery.
Ocular stress
An ophthalmologist assessed surgeons for stereoscopic vision and to exclude manifest strabismus using five qualitative and semi-quantitative tests: Lang I and II, Titmus, Bagolini, TNO, and cover/uncover tests. Monocular visual acuity was measured, and both the anterior segment and central fundus were screened for relevant anomalies. Visual defects were also investigated.
The impact of operating theater workload on vision was evaluated with dedicated tests, including direct measurement using the 2WIN infrared binocular autorefractometer (Adaptica srl, Italy). This device is a portable binocular video refractometer and vision analyzer that measures both eyes simultaneously under real-world conditions, detecting refractive errors, eye abnormalities, and vision problems across a range of −15D to + 15D. It also assesses dynamic pupil responses to light and lens centering, identifying myopia, hyperopia, astigmatism, amblyogenic factors, anisometropia, anisocoria, strabismus, and phorias.
Indirect measures of binocular vision were performed using T.N.O. tables, Berens prism sticks, Facchin Card, Wesson Card, and Saladin Card (C.O.I. srl, Termoli, Italy).
Mental workload
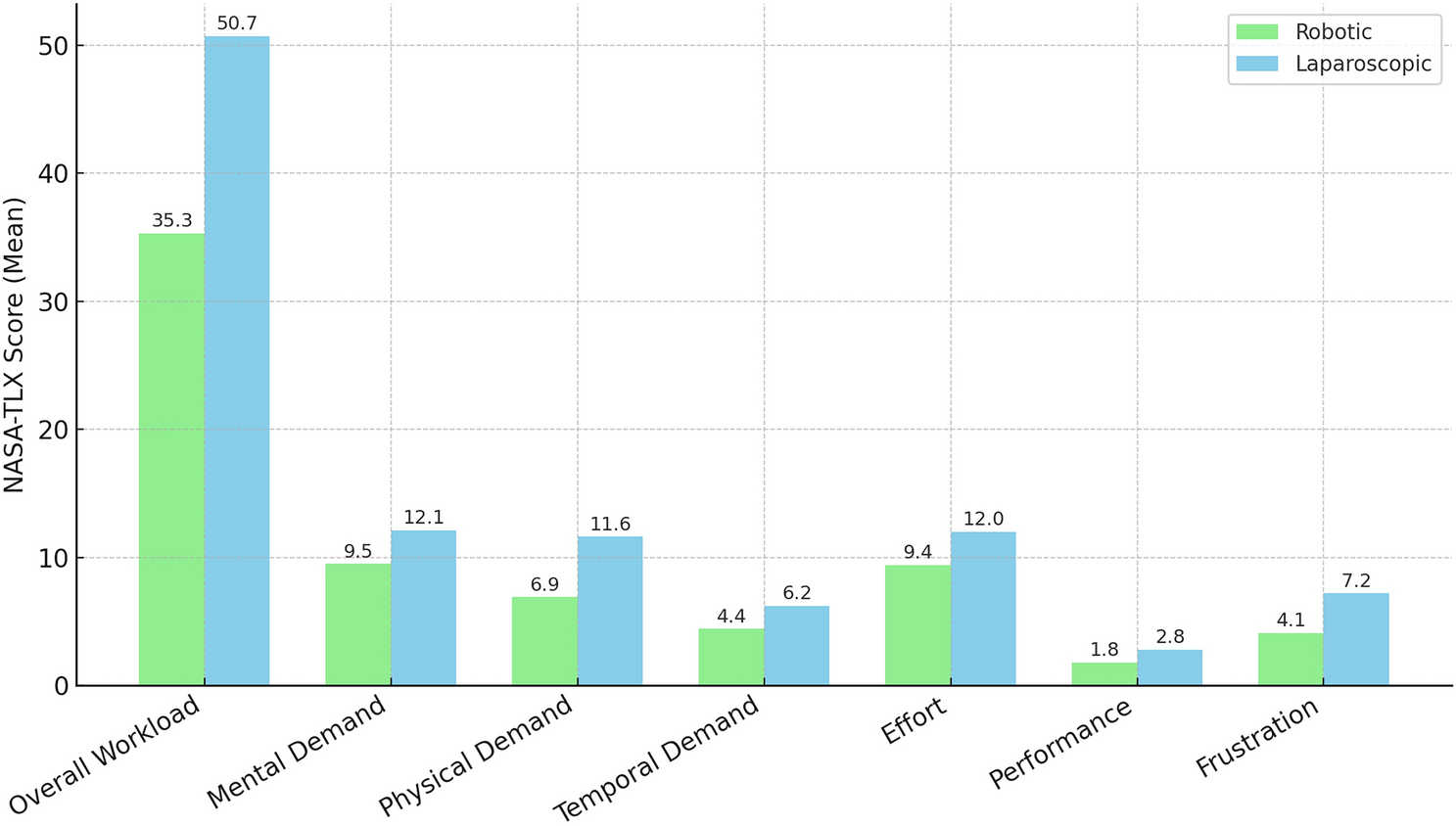
The NASA Task Load Index (NASA TLX) was used to evaluate subjective mental workload [14]. It assessed six domains: mental, physical, temporal, effort, performance, and frustration. Participants rate each domain on a 20-point scale (0 = low, 20 = high), while performing a task. An overall workload score was calculated, with a midpoint threshold for overload set at 49.5 out of 100. For individual subscales, a midpoint threshold of 9.5/20 was used for rounding [15] (Appendix 1).
Cortisol parameters
Surgeons collected saliva six times daily for baseline values: upon waking, at 8:00 AM, 12:00 PM, 3:00 PM, 7:00 PM, and at 11:00 PM, using Salivette Tubes (Sarstedt, Nümbrecht, Germany). Participants were instructed to avoid alcohol for 48 h, intense exercise for 24 h, and eating, drinking (except water), smoking, or oral hygiene for 1 h before each collection. Intraoperative sampling was performed immediately before the incision, every 2 h during surgery, and at the conclusion. Detailed sample analysis is reported elsewhere [16].
Operations
Laparoscopic DP was performed using the IMAGE1 S Rubina surgical system (Karl Storz, Tuttlingen, Germany); robot-assisted DP utilized the da Vinci® Si surgical system (Intuitive Surgical, Sunnyvale, CA, USA). Patients with pancreatic body/tail lesions treated with DP were evaluated at the authors’ institution. Laparoscopic DP (LDP) and robotic distal pancreatectomy (RDP) were performed as previously described [17, 18]. In LDP, the patient is placed in the supine position with a 20–25° reverse Trendelenburg tilt and a 15–20° right lateral tilt. The first 12 mm trocar is inserted above the umbilicus for the camera. A 5-mm trocar is then positioned in the epigastrium beneath the left costal margin. A third 5-mm trocar is inserted in the right hypochondrium along the midclavicular line, above the transverse umbilical line. Finally, a 12-mm port is placed in the left hypochondrium, lateral to the umbilicus along the midclavicular line. An additional 5 mm port may be added more laterally in the left hypochondrium to enhance exposure. In RDP, five trocars are used: four 8 mm robotic ports along a transverse line at the umbilicus level (R1 in the right flank, R2 in the right pararectal area, R3—camera—in the periumbilical region, R4 in the left flank), and a 12 mm assistant port positioned below and between R3 and R4. A standard distal pancreatectomy with splenectomy and lymphadenectomy was performed for malignant lesions. For pancreatic body and tail tumors suspected of posterior margin involvement, radical antegrade modular pancreatosplenectomy was performed. When addressing benign tumors, spleen preservation was always attempted. Regarding the technique of transection, the triple-row stapler reinforced with a PGA felt (NEOVEIL Endo GIA Reinforced Reload with Tri-Staple® Technology 60 mm, COVIDIEN, North Haven, CT, USA) was used [19]. The surgical field was drained using a Penrose-type drain placed proximal to the pancreatic remnant. Postoperatively, the drain was managed according to the institutional protocol[20].
Statistics and sample size
Given the exploratory design, a sample size assessment was not performed. Twenty procedures were deemed sufficient to assess the workload in laparoscopic and robot-assisted DP.
Normally distributed continuous variables were compared using the two-sample t-test (means ± SD). While non-normally distributed variables were analyzed using the Mann–Whitney U test (medians and interquartile ranges, IQR), Categorical variables were assessed using chi-square or Fisher’s exact test (proportions). Statistical significance was set at p < 0.05 (two-tailed). Variables with p < 0.10 in univariable analysis were included in multivariable regression.





Comments (0)