In this 5-year retrospective study of inpatient hereditary thrombophilia testing after acute VTE, we found that abnormal results were very common and rarely changed clinical management. These findings highlight a disconnect between current practice and most evidence-based recommendations. Testing was frequently performed immediately following a VTE event, when results are more likely to be misleading, and was associated with significant costs.
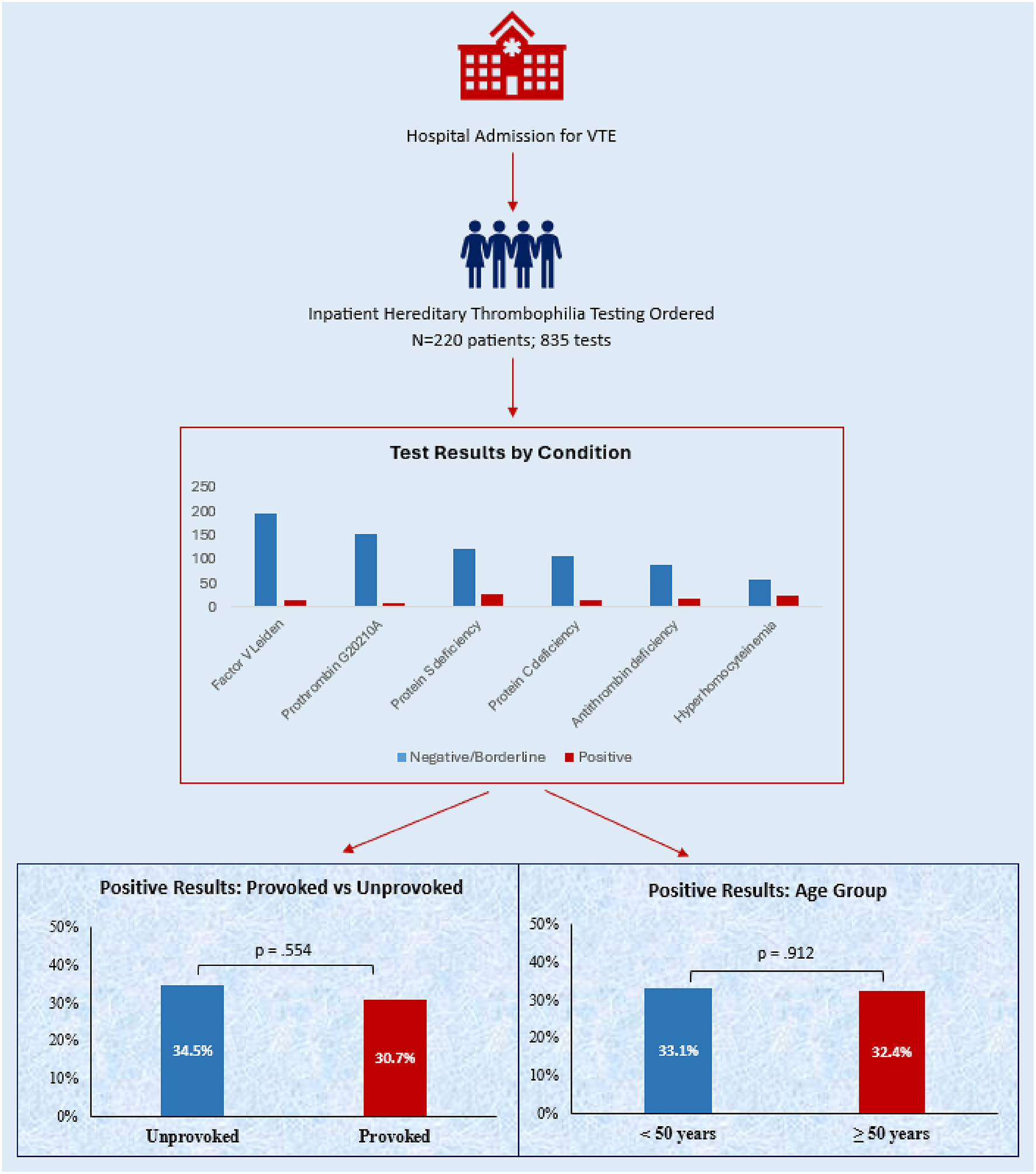
First, our study found a high rate of test utilization in groups for whom hereditary thrombophilia testing has not been recommended. British Society for Haematology guidelines advise against routine thrombophilia testing when results are unlikely to affect clinical management decisions [21]. These further note that the presence of hereditary thrombophilias rarely alters intensity, choice, or monitoring of anticoagulant therapy, and instead emphasize using clinical history and assays such as D-dimer in selected patients to guide management [21]. Similarly, ASH Choosing Wisely® recommendations include not ordering thrombophilia tests after VTE by a major risk factor [20]. However, multiple studies have reported high rates of thrombophilia testing after a provoked VTE [13,14,15, 26,27,28,29]. Our study similarly found testing following provoked VTE was very common, comprising 45.9% of our patients and 47.3% of total tests. Even excluding VTE provoked by pregnancy or estrogen – a group for whom recent ASH guidelines support testing [22] – 29.5% of patients had a provoked VTE. Furthermore, while some advocate for selective thrombophilia testing in young patients and those without a strong provoking risk factor [30], we found that the rate of positive tests was not significantly greater in patients with unprovoked as compared to provoked VTE, nor in patients younger than 50 years of age or those with recurrent VTE.
The utility of thrombophilia testing is further limited by the potential for false positives when ordered in the acute setting, which our study confirmed. Testing following acute VTE is more likely to yield false positive results due to anticoagulation therapy that affects certain functional assays, protein consumption by acute thrombus or mechanical circulatory support systems, or acute phase reactant changes related to inflammation and/or the predisposing condition to VTE [10, 11, 26, 31]. We found 21.9% of antigen and functional assays with a lower limit of normal of 70% or higher yielded results below normal but above typical values in autosomal dominant deficiency, indicating a high likelihood of being a false positive. This has the potential to yield mismanagement of patients when results are misinterpreted or not repeated.
Furthermore, we found that fewer than 10% of patients with an abnormal antigen or activity assay had repeat testing for confirmation after the hospitalization. Others have found that while abnormal tests may be repeated, it is often during the index admission, when false positive results are still likely [15]. By focusing solely on inpatient testing after an acute VTE event, our study adds to the current literature by highlighting the importance of timing in performing hereditary thrombophilia testing. Given the high rate of likely false abnormal results and low rate of test repetition for confirmation, our data suggests that clinicians should defer testing to after an acute VTE and that guidelines such as those from ASH should directly address timing of testing in order to reduce confounding variables and the risk of clinical mismanagement of patients.
The management of patients in our study reflects that clinicians likely viewed the test results with skepticism. Only 4% of patients with any abnormal result had a documented change in clinical management in response to an abnormal result. This is consistent with other studies which found that inpatient thrombophilia testing was not clinically useful or reliable and rarely changed management [13, 14, 27, 28]. Additionally, many of these studies included acquired thrombophilias such as antiphospholipid syndrome, which often requires a change in anticoagulant – specifically to warfarin – and thus may be a higher yield test to order, especially in patients for a whom a high clinical suspicion exists. One single-center study, for example, found that 87% of patients were tested inappropriately and in no cases was the duration of treatment impacted by the result. However, among the 7 patients who experienced any clinical change in management, all had antiphospholipid syndrome, which was not included in our study [14]. Together with our study, this reinforces the concept that these tests rarely provide valuable data that impacts treatment decisions.
Finally, thrombophilia testing is expensive. When these tests are used inappropriately, they offer minimum clinical benefit but also contribute to significant spending, which may be costly to health care systems when ordered in the inpatient setting [13, 15, 26, 29]. Although cost-analysis of thrombophilia testing in acute VTE is sparce, estimates for the panel of tests included in our study range from approximately $187 to $974 USD per patient [14, 15, 26, 28, 32]. To provide a broad estimate of costs, we calculated charges using both our institution’s chargemaster and the most recent publicly available CMS fee schedule. In our study, the total institutional charges by chargemaster were greater than $385,000 USD and by CMS fee schedule greater than $26,000 USD over the 5-year study period. The corresponding per-patient charges were $1,750 and $118 USD, respectively. The implication of our findings is that reducing the utilization of these tests – or limiting them to guideline-recommended situations – represents a potential cost savings opportunity for the US health care system.
Our study has certain limitations. The retrospective, observational design from a single academic hospital system may limit the applicability of our findings to other institutions or patient populations. Additionally, the reliance on reviewing documentation to understand clinical outcomes and indications for therapy represents a weakness. Incomplete documentation, particularly from outside our EHR system, restricted our ability to fully understand and assess outcomes and potential changes in management. Many patients had no documented encounters after hospital discharge, which limited our ability to assess long-term clinical management, but also highlights the low yield of thrombophilia testing when ordered inpatient. To mitigate challenges due to incomplete documentation, charts were reviewed independently by both members of our study team, and the median time from testing to the last VTE-related documentation was 215 days, indicating extensive follow-up for many patients. Another limitation is that our study did not specifically measure the percentage of patients who were receiving anticoagulation – and which agent was being used – at the time of thrombophilia testing, which would have provided insight into reasons for false positive results. It is noted, however, that most patients had been started on anticoagulation before testing was ordered. Important strengths of this study include its use of real-world data and long study period and follow-up time, which can add valuable insights into clinical practice around thrombosis care – especially in the acute care setting – and we feel may inform future guidelines, especially those addressing the timing of testing.


Comments (0)