
Remember me

Optimal duration of anticoagulant treatment in patients with CRT-UEDVT is unclear. As mentioned above, there are data from a systematic review showing that 3% of patients have recurrent VTE during a median follow-up of 13 months [18]. Other data from the RIETE registry indicate that the annual recurrence incidence of thrombosis after discontinuing anticoagulation is approximately 1.5% [16]. It is usually recommended to continue anticoagulation until the catheter is in place [24], and patients with cancer, who are the majority of those with CRT-UEDVT, should be kept on anticoagulant therapy until the cancer remains active and/or cancer treatment is ongoing [13]. The result is that many patients with CRT-UEDVT are kept on anticoagulation not just for the treatment of the thrombosis itself, but because the CVC is still in place and/or they have active cancer. The net clinical benefit of such extended anticoagulant regimens is unknown. It is also unknown whether DOACs, especially those at reduced dose, may be effectively and safely used in these patients since the studies on reduced-dose DOACs for extended treatment have not included patients with CRT and UEDVT [25,26,27]. In the present study, we assessed effectiveness and safety outcomes associated with different lengths of anticoagulation, focusing on women with active cancer and CRT-UEDVT. We decided to focus on women because they are often underrepresented in thrombosis research, particularly in randomized controlled trials and registries [28].
Fig. 1
Anticoagulation regimens in the study population at 3, 6 and beyond 6 months. DOAC, Direct Oral Anticoagulant
Fig. 2
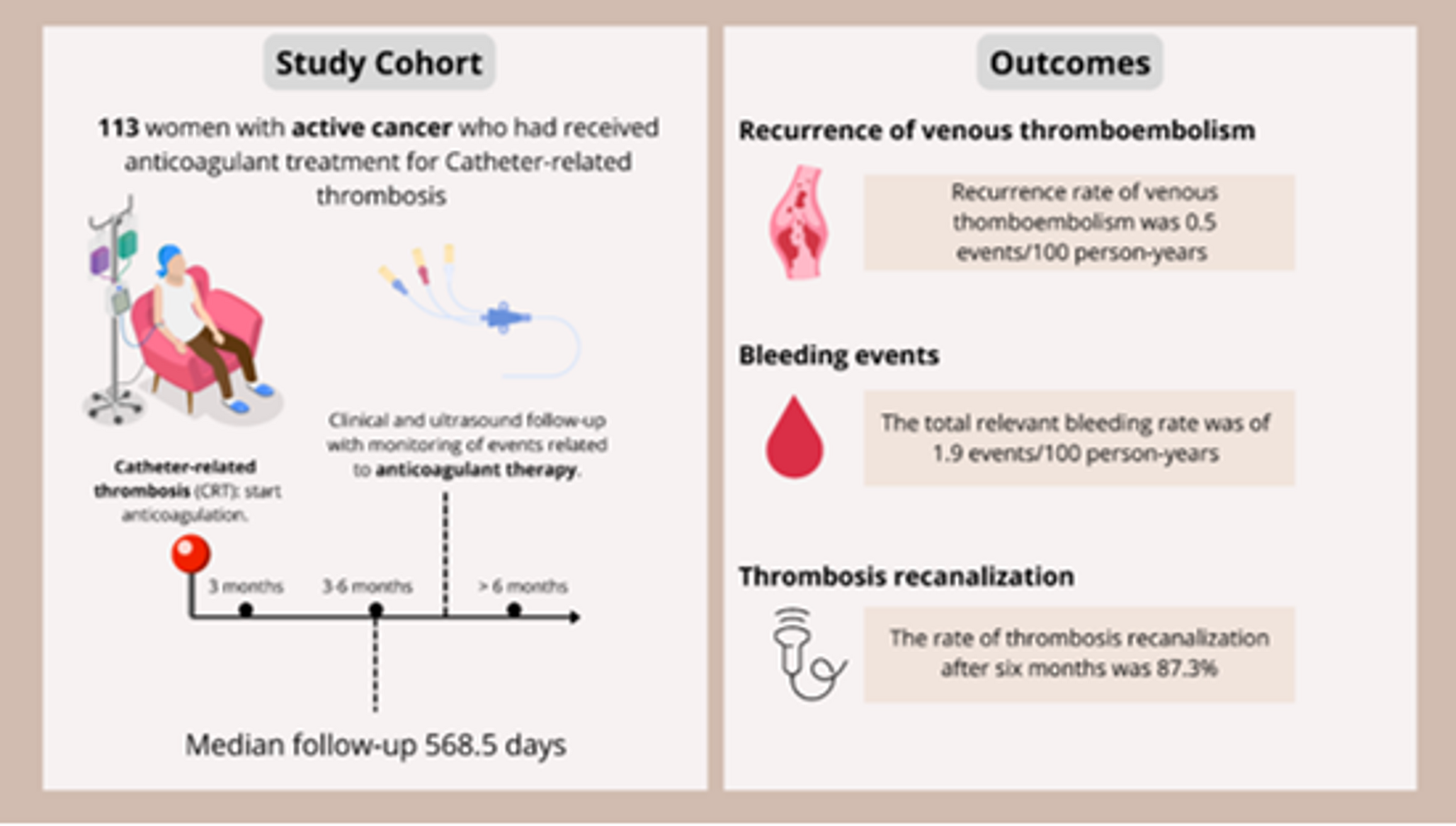
Thrombosis recanalization in the study population assessed by Doppler ultrasound at 3, 6 and beyond 6 months
Regarding the management of CRT-UEDVT, we found that most patients received parenteral anticoagulation during the first three months, with a smaller proportion receiving DOACs. The use of parenteral anticoagulation in the first months is consistent with current guidelines for cancer-associated VTE, where LMWH is often the first-line therapy [13, 29]. However, the use of DOACs in a smaller subset of patients reflects a growing interest in their role in cancer-related thrombosis, though more research is needed to determine their safety and efficacy compared to traditional parenteral therapies in this clinical entity [30].
Regarding VTE recurrence, its annual rate in our study was 0.5%, which is lower than previously reported in the literature among patients with UEDVT [18, 19]. It is also lower than the rate of recurrence documented in patients who are on extended anticoagulation because they had a DVT in a usual site (proximal deep veins of the legs and/or pulmonary embolism) [19, 31,32,33]. These findings suggest that extended anticoagulation protects cancer patients with CRT-UEDVT from thrombotic recurrences in the long term and is consistent with the notion that extended anticoagulation significantly reduces the risk of VTE recurrence in cancer patients [34]. It is interesting to note that these results were obtained in patients who were mainly treated with DOACs at reduced doses (84.5% of patients) in the time lapse 6–12 months.
Regarding MB and CRNMB, their annual rate in our study was 1.9%, which is higher than the annual incidence of VTE recurrences. This finding indicates that the potential beneficial effects of extended anticoagulation in terms of effectiveness are not free from haemorrhagic events in women with cancer, even if they are treated with low doses of anticoagulants. Our data are consistent with notion that bleeding remains a relevant concern in patients with cancer, particularly as they prolong anticoagulation over an extended period [35, 36]. Among the results of our study, it is interesting to note that anticoagulant treatment beyond 3 months was associated with a greater extent of complete recanalization of the index thrombotic event. This finding suggests that extended anticoagulation may have beneficial effects on this specific effectiveness outcome.
A strength of this study is the notably long median follow-up duration of 568.5 days, which allowed for the evaluation of clinical outcomes in the long term. The focus on female patients is a strength, since women are often underrepresented in clinical trials and observational studies and this can lead to lack of understanding of sex-specific differences in thrombotic and haemorrhagic risks, as well as effectiveness and safety of antithrombotic treatments in women. Moreover, the heterogeneity of cancer sites offers a representative overview of the female oncology population.
This study has some limitations that should be acknowledged. Its retrospective, observational, and monocentric design inherently limits the generalizability of the findings and may introduce potential biases. The allocation of patients to different anticoagulation durations was unbalanced, with most participants receiving long-term therapy. Similarly, different classes of anticoagulants were used, and frequent treatment modifications occurred during the follow-up period. This heterogeneity complicates the interpretation of outcomes and may act as a confounding factor. In addition, venous Doppler ultrasonography was performed in a relatively limited number of patients, which may restrict the accuracy of the assessment. Finally, the inclusion of male patients could have increased the sample size and enabled the investigation of potential sex-related differences with greater statistical significance.
Nevertheless, our study thus provides unique insights into the way women with cancer and CRT-UEDVT are therapeutically managed and how their outcomes are.
In conclusion, the findings of our retrospective cohort study suggest that, in female patients with cancer and catheter-associated thrombosis, a 3-month course of anticoagulant therapy may be sufficient to achieve thrombotic recanalization, while maintaining an acceptable safety profile. Given the low incidence of thromboembolic recurrence and the non-negligible risk of bleeding, the decision to extend anticoagulant therapy beyond this period and its dose warrants careful, individualized consideration. Finally, DOACs appear to be a valuable therapeutic option in this patient population.
Comments (0)