BCR-ABL TKI therapies for chronic myeloid leukemia (CML)
Imatinib is a first generation BCR-ABL TKI used in the treatment of chronic myeloid leukaemia (CML). It has been well studied for almost two decades and has showed minimal vascular risk. However, studies of both second and third generation agents have demonstrated significantly higher thrombotic events. In the Evaluating Nilotinib Efficacy and Safety in Clinical Trials—Newly Diagnosed Patients (ENESTnd) trial comparing nilotinib to imatinib for newly diagnosed CML, cardiovascular events (coronary, cerebrovascular, or peripheral arterial) were markedly more frequent with nilotinib. At 3 years, arterial event rates were ~3–4% with nilotinib versus 2.1% with imatinib, and by 6 years the rates increased to 7.5% and 13.4% in the nilotinib 300 mg BID and 400 mg BID arms, respectively (versus 2.1% on imatinib) [55]. These late-emerging arterial occlusions with nilotinib often involved severe peripheral arterial disease requiring revascularization and are considered due to both thrombotic events and worsening of atherosclerotic disease [56, 57].
Ponatinib, a potent pan-kinase inhibitor, has an even more striking thrombotic profile as was demonstrated in the Ponatinib Ph-positive acute lymphoblastic leukemia [ALL] and CML Evaluation (PACE) trial for refractory CML. Ponatinib led to serious arterial thrombotic events in ~20% of patients over 5-year follow-up. In part, this is believed to be due to off target effects of treatment inhibition of VEGF and FGF receptor pathways [58]. These included cardiovascular (10%), cerebrovascular (7%), and peripheral arterial events (8%) [13].
The risk was dose-dependent, prompting dose reduction strategies and a “black box” FDA warning along with Ponatinib now more frequently considered a second line treatment strategy [10]. A subsequent front-line trial found similar compelling results when comparing ponatinib to imatinib and was terminated early (after ~5 months) when 7% of ponatinib treated patients experienced arterial occlusive events, majority of these where deemed severe [14].
Notably, other CML TKIs like dasatinib and bosutinib have not shown such high rates of arterial thrombosis; the risk seems particularly elevated with nilotinib and ponatinib, possibly related to their multi-kinase activity and metabolic effects.
Angiogenic TKIs
Another group of TKIs which have raised similar concerns of thrombosis have been those targeting VEGFrs in solid tumours (e.g., sunitinib, sorafenib, pazopanib, axitinib). The mechanism of arterial thromboembolism is considered to be likely via endothelial effects and hypertension, as opposed to progression of atherosclerotic disease [25, 44]. A meta-analysis of trials including over 10,000 patients assessed VEGF-pathway targeted agents (Sunitinib and Sorafenib) and found a roughly threefold increased relative risk of arterial thrombotic events compared to controls [25]. In that analysis, the overall incidence of arterial events (such as myocardial infarction or stroke) was still relatively modest (in the order of a few percent), but clearly higher than in placebo/controls [25]. Similarly, two other large meta-analysis of various VEGF inhibitors (VEGFi) reported a modest range (2.8–3.5) relative risk increase of myocardial ischemia amongst treated patients [59, 60].
The FDA has also documented arterial thromboses with other VEGF/PDGF inhibitors and related agents such as pazopanib, regorafenib, lenvatinib, and even some endothelial growth factor receptor (EGFR) TKIs and monoclonal antibodies [46, 61].
Thus, any agent impairing angiogenesis signals can potentially precipitate arterial ischemic events, although the absolute risk for an individual patient remains fairly low (generally <5%). Risk factors (like pre-existing cardiovascular disease) greatly modulate the absolute risk.
Non-angiogenic TKIs and others
Some newer targeted TKIs have less evidence of thrombosis, but isolated signals exist. BTK inhibitors (e.g., ibrutinib for B-cell malignancies) are primarily associated with bleeding (see next section) rather than thrombosis; however, they do predispose patients to atrial fibrillation in up to 10–16% of cases. This indirectly increases stroke risk if not managed [62].
Anaplastic lymphoma kinase (ALK) inhibitors (crizotinib, alectinib) and other modern TKIs have not shown strong thrombosis signals in trials, aside from events attributable to the cancer itself [10].
It is important to distinguish arterial vs. venous risk. Interestingly, TKIs that markedly increase arterial thromboses do not always confer a similar increase in venous clots. The VEGFR inhibitor class, for instance, shows a clear arterial risk, but a more equivocal effect on venous thromboembolism (VTE). A 2013 meta-analysis of >4400 patients on VEGFR-TKIs (sunitinib, sorafenib, pazopanib, vandetanib) found an overall VTE incidence of ~3% on these TKIs, and no statistically significant increase in VTE risk compared to patients on non-TKI therapy [23]. The relative risk of VTE with VEGFR-TKIs was ~0.91, found to be essentially neutral [63]. This suggests that cancer type and patient factors (e.g., immobility, pro-coagulant tumours) are the dominant drivers of VTE, rather than the TKI itself. In contrast, arterial events seem more directly attributable to certain TKIs’ pharmacologic effects on vessels and platelets [64]. The key point is that not all TKIs confer the same thrombotic risk profile.
In summary, each TKI (and class of TKIs) has a distinct thrombotic “fingerprint”. Clinicians should familiarize themselves with the specific risks of the TKI being prescribed. For example, a patient on ponatinib needs aggressive cardiovascular risk factor management and monitoring for arterial ischemia, whereas a patient on ibrutinib needs monitoring for atrial fibrillation and might actually have a reduced platelet aggregation tendency. Understanding these nuances allows for personalized preventative strategies and prompt recognition of thrombosis if it occurs.
Bleeding and platelet inhibition associated with TKIs
Targeted tyrosine kinase inhibitors (TKIs) have improved efficacy over conventional chemotherapy [65]. However, these agents are associated with significant adverse effects in several trials and case reports, including an increased risk of bleeding and platelet inhibition [30, 51]. A better understanding of the mechanisms underlying bleeding and platelet dysfunction is crucial to develop a personalised method to improve patient outcomes [66, 67].
VEGFR-TKIs have improved outcomes for certain types of solid tumours [68]. However, one of the common side effects of VEGFR-TKIs is increased risks of bleeding and platelet aggregation inhibition as well as thrombocytopenia [69,70,71,72].
A meta-analysis of 23 trials that included 6779 patients reported that 708 out of 4934 patients (16.7%, 95% CI 12.7–21.5%) treated with VEGFR-TKIs had all grades of bleeding events, whilst high-grade bleeding events (defined as ≥grade 3, based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events) occurred in 100 out of 6597 patients This represents an incidence rate of 2.4% (1.6–3.9%) [73]. According to data from phase III trials, the use of TKIs (sunitinib and sorafenib) presented a twofold increase in the risk of all-grade bleeding events (95% CI, 1.14–3.49; p = 0.015) [73]. There was no statistical significance observed between renal cell cancers and non-renal cancers [73].
Another meta-analysis of 27 randomised controlled trials demonstrated that the use of VEGFR-TKIs was consistently associated with increased haemorrhagic events by 67% (RR 1.67, 95% CI 1.19–2.33, p = 0.003) [74]. Though the overall incidence of all grade and high-grade haemorrhagic events was lower at 9.1 and 1.3%, respectively [74].
Furthermore, a broader network meta-analysis included 50 RCTs of 16,753 cancer patients and analysed bleeding profiles for eleven U.S. FDA approved VEGFR-TKIs (Apatinib, Brivanib, Cabozantinib, Lenvatinib, Motesanib, Nintedanib, Pazopanib, Regorafenib, Sorafenib, Sunitinib and Vandetanib) [75]. Looking at all-grade bleeding events, 1283 of 9575 patients receiving VEGFR-TKIs were at an increased bleeding risk compared to 617 of 7178 patients in the control group [75]. The risk of high-grade bleeding was not significantly increased in VEGFR-TKIs group (RR 1.22; 95% CI 0.87–1.71, p = 0.74)[75]. Interestingly, sunitinib (Odds Ratio, OR = 3.31, 95% CI 2.34–4.69) and regorafenib (OR = 2.92, 95% CI 1.50–5.71) showed a significantly higher risk of haemorrhagic events compared to placebo [75].
Cancer induces a hypercoagulable state [76, 77]. It is critical to balance the benefit and risk between bleeding and thrombosis. Low-molecular-weight heparin (LMWH), an indirect factor Xa inhibitor, has been the standard treatment for cancer-associated thrombosis for the past decade [77,78,79,80]. Clinical trials, including the Randomized Comparison of Low-Molecular-Weight Heparin versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer (CLOT) [81] and Comparison of Acute Treatments in Cancer Haemostasis (CATCH) trial [82], have demonstrated its efficacy in preventing recurrent venous thromboembolism in cancer patients. However, LMWH carries an increase in major bleeding risk ranging from 2.7 [82] to 6% [81].
A retrospective study of 86 patients with cancer receiving VEGFR-TKIs (pazopanib, sunitinib, sorafenib, axitinib, regorafenib, vandetanib, lenvatinib, or cabozantinib) and factor Xa inhibitors (LMWH or DOACs) [83] found that concurrent use of VEGFR-TKIs and factor Xa inhibitors (primarily LMWH) increases the risk of clinically significant bleeding events in patients with metastatic cancer (hazard ratio, HR 2.45; 95% CI, 1.28–4.69, p = 0.007). In addition, a retrospective study of 258 individuals did not detect a significant difference in their primary outcome, defined as rates of major bleeding in VEGF TKI plus anticoagulation compared to VEGF TKI without anticoagulation (8% vs 3%, p = 0.095). However, in this study a higher bleeding risk was noted in the composite endpoint of major and minor bleeding (OR, 2.73; 95% CI, 1.36–5.46; p = 0.005) [64]. This underpins the importance of nuanced clinical decision making in these at-risk groups.
Another retrospective study [84] of 100 patients with chronic myeloid leukemia (CML) found that those with TKI treatment (imatinib, dasatinib, nilotinib, bosutinib, or ponatinib) and selective serotonin reuptake inhibitors (SSRI) had a statistically significant higher incidence of critical site major bleeds compared to those without SSRIs. In addition, bleeding risk appears to depend on the specific TKI, as all observed bleeding events occurred in those with imatinib or dasatinib [84]. However, the risk of major bleeding or thrombotic events were similar. Previous studies reported substantial interindividual variability in the effects of different TKIs [85].
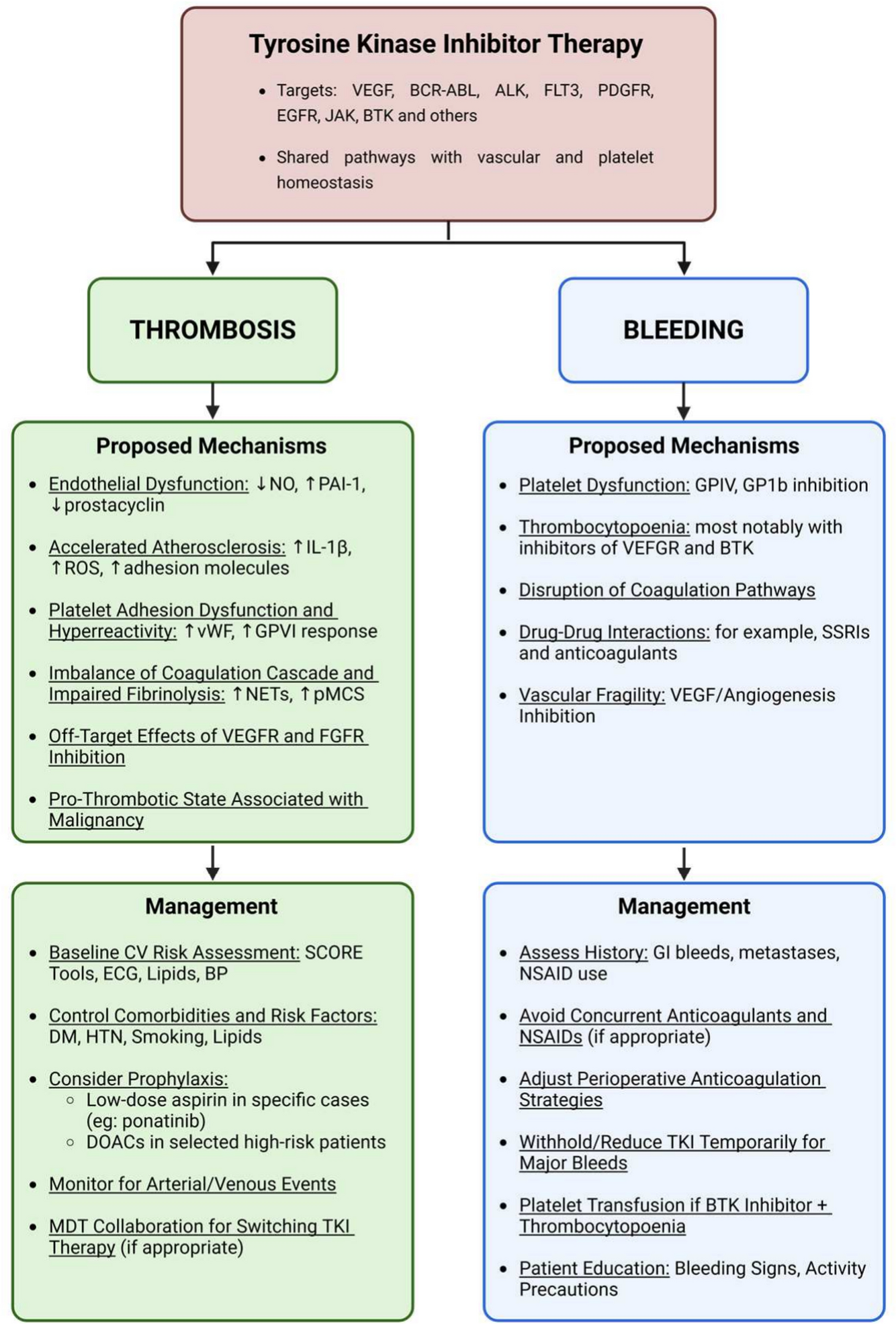
Current and emerging TKIs play a role in platelet activation and signalling pathways through off‐target effects [71]. These include pathways downstream of: (1) the immunoreceptor tyrosine-based activation motif (ITAM)-associated receptor glycoprotein VI (GPVI), (2) integrins such as αIIbβ3, (3) G protein-coupled receptors (GPCRs), and (4) the Janus kinase (JAK)/signal transducer and activator of transcription (STAT) signalling pathways [86]. However, the mechanism of BTK inhibitors on platelet function and haemostasis is unclear. Previous studies [87,88,89] suggested that GP1b and GPVI signalling pathways of the platelet receptors contributed potential bleeding events from ibrutinib. Patients who had mild bleeding do not require BTK inhibitor discontinuation [88], but if major bleeding occurs temporary cessation is advised [90]. To minimise the risks of perioperative bleeding, ibrutinib dose adjustment or urgent platelet transfusion should be considered [62, 88, 91].
Management strategies for TKI-related thrombosis and bleeding
The balance of risk between thrombosis and bleeding in cancer patients on TKI therapy poses a significant clinical challenge for all practitioners involved in a patient’s cancer and cardiovascular care. This in turn means providers must look to prevent thrombosis, and at times treat thrombosis, whilst also considering risk reduction for major bleeding events and vice versa. Therefore a collaborative multidisciplinary approach is favoured, often involving medical and radiation oncologists, haematologists, cardiologists and primary care practitioners with a focus on individualised patient centric care [92].
Baseline risk assessment
Before TKI initiation the utilisation of guideline directed cardiovascular (CV) risk assessment is essential, which now must also include an assessment of bleeding risk [40]. Risk factors for thrombosis may include; history of coronary or peripheral artery disease, stroke, diabetes, smoking, hypertension, hyperlipidaemia, as well as prior venous thromboembolism or hypercoagulable conditions [40, 93]. For bleeding, consider any history of bleeding disorders, peptic ulcer disease, malignant metastases in crucial areas such as the bowel, liver or brain, use of non-steroidal anti-inflammatory drugs (NSAIDs), concurrent indications and use of anticoagulants, or severe thrombocytopenia [94]. This upfront assessment can guide preventative strategies and allow informed open discussion with patients about their individualised risk.
Modification of identified risk factors
Aggressive management of modifiable risk factors in patients receiving TKIs, especially those known to increase thrombosis, is a crucial step towards prevention. Patients on pro-thrombogenic TKIs should have optimal control of blood pressure, cholesterol and blood sugar, and they should be advised on smoking cessation and regular exercise [95]. Risk factor modification also extends to individual bleeding risk—for example, patients should be made aware and in cases avoid concomitant non-vital medications that can compound bleeding (NSAIDs, fish oil supplements, etc.), and ensure good blood pressure control to reduce the risk of haemorrhagic strokes.
Prophylactic antithrombotic therapy
Whether to use prophylactic antiplatelet or anticoagulant therapy in patients on TKIs is a nuanced decision. There is no one-size-fits-all guideline, and it must be individualized. Limited evidence already exists in the use of novel oral anticoagulant (NOACs) with low dose apixaban in select patients with high-risk cancer, with low-dose Apixaban demonstrating effective decrease the likelihood of venous thromboembolism despite the use TKIs [96]. Additionally, for high-risk patients receiving ponatinib, a preventive approach involving low-dose aspirin (100 mg/day) has been advised for individuals aged 60 years or older to mitigate the risk of arterial occlusive eventsv [97]. However, as suggested above the balance is complex and both prophylactic measures may elevate the potential for bleeding complications.
Another consideration is in patients taking the TKI ibrutinib who subsequently develop atrial fibrillation, guidelines suggest anticoagulation for stroke prevention should be instituted but typically a direct oral anticoagulant (DOAC) is preferred over warfarin in this scenario (warfarin has commonly been avoided in ibrutinib trials due to bleeding concerns) [98]. In fact, evidence suggests DOACs may be safer to combine with TKIs than vitamin K antagonists. A retrospective study found that among patients on VEGFR-TKIs who needed anticoagulation, those on DOACs had bleeding rates comparable to those on LMWH or warfarin [64]. Thus, if anticoagulation is necessary, DOACs are generally the first choice (provided no contraindications like gastrointestinal cancer bleeding risk or drug–drug interactions).
Patient education, monitoring and early detection
Educating patients about the signs and symptoms of both thrombosis and bleeding could be potentially lifesaving and cannot be overemphasized. Patients on TKIs need to know how to identify these complications, and to seek immediate care for symptoms of stroke or heart attack, as well as report any significant bleeding [93, 99]. They should be instructed on lifestyle modifications (using a soft toothbrush, an electric razor for those at risk of bleeding, avoiding high-risk activities such as heavy contact sports if platelets are low) [100]. Education should also cover medication interactions that could worsen bleeding, and informing all providers (including primary care practitioners and dentists) that they are on a TKI that affects bleeding/thrombosis.
Patients on TKIs should be regularly monitored for signs of thrombosis and bleeding. This includes periodic clinical assessment and appropriate investigations. This may include opportunistic review in clinic or at cancer treatment centres. Furthermore, a collaborative approach with the multidisciplinary team including involving nurse practitioners in these assessments will likely increase diagnostic yield and improve patient outcomes. Ideally monitoring for both thrombosis and bleeding should also extend beyond the hospital and treatment setting to also encompass the central role that primary care practitioners play in a patient’s cancer journey.
Managing a thrombotic event
If a patient develops a thrombosis whilst on a TKI, management typically involves treating the thrombosis as per standard treatment protocols (e.g., anticoagulation for venous thromboembolism (VTE), antiplatelet therapy for strokes and peripheral vascular disease and dual antiplatelet therapy and possible stenting for acute myocardial infarction (AMI)). In the acute setting, temporary interruption of the TKI is often advisable until the clinical situation and treatment plan is established [51]. For example, in AMI patients TKI may be withheld initially in discussion with the patients cancer care team given the TKI could complicate interventions if it causes platelet issues or the patient needs surgery. Following longer-term decisions will need to be made between the multiple specialists (Cardiologist, Oncologists, Haematologist) and the patient to determine the safety of TKI resumption and secondary preventative strategies. If the thrombosis is clearly attributed to the TKI, switching to an alternative cancer therapy with less thrombotic risk is prudent if feasible. In CML, for instance, a patient who suffers a serious arterial event on ponatinib might be transitioned to asciminib or back to dasatinib (balancing cancer control vs risk). If no alternative exists and the TKI is essential, then secondary prophylaxis with antithrombotic therapy may be instituted along with close monitoring [101]. In all cases, a tailored collaborative approach is key where there is a paucity of evidence. Studies in mice and case reports of patients experiencing arterial occlusive events while on ponatinib have explored the use of N-acetylcysteine and pioglitazone as potential interventions [102]. LMWHs have been the standard of care for treating arterial and venous thrombosis until the revolution of DOACs which in most cases are proven as effective as LMWH, however, this marginally increased the rate of major bleeding. This prevention strategy may not be applicable in patients with thrombocytopaenia due to the significant increase in major bleeding.
Managing a bleeding event
If significant bleeding occurs on a TKI, holding or stopping the TKI is usually the first step. Further supportive measures are often dictated by bleeding severity and reversibility. For mild bleeding (for example Grade 1–2 epistaxis), local measures and temporarily withholding the drug may suffice [51, 103]. Often the TKI can be resumed at the same dose once bleeding has resolved [51]. For more serious internal bleeding (for example an intracranial haemorrhage), the TKI should be stopped, and standard critical care for bleeding is required in discussion with appropriate oncological and haematological consultation [51, 103]. This may include blood product support (packed red blood cells, platelet transfusions if thrombocytopenic or suspected platelet dysfunction), cautious use of haemostatic medications (such as tranexamic acid), and urgent intervention (endoscopy, interventional radiology or surgery) as needed. Platelet transfusion is an important consideration for BTK inhibitor TKI treated patients with major haemorrhage given that ibrutinib causes irreversible BTK binding in existing platelets, transfusing new platelets can partially restore haemostatic function [91]. Of note, ibrutinib has a relatively short plasma half-life (~6 h), thus drug levels decline quickly and often withholding the drug and supporting the patient for a day or two can allow restoration of platelet function as new platelets are made [86, 91].
Decisions around resuming the TKI after a serious bleed are complex an often switching to alternatives therapies of a different class should be considered [91]. If the informed decision is made to restart a TKI, the specialists involved may decide on a dose-reduction if possible and ensure all reversible bleeding risk factors are also addressed [51].
Coordination of care a collaborative balanced approach
As highlighted above, involvement of a multidisciplinary team is invaluable and allows for improved patient outcomes across the spectrum of cardio-oncology care [104]. The collaborative approach including the Cardiologist or Cardio-oncologist, Haematologist, Medical and Radiation Oncologists, Primary Care Practitioners along with the nursing and allied health teams allows for informed decision making between multiple specialised fields alongside the patient throughout their cancer journey [104]. Complex decisions around TKI treatment risks, prevention and management of possible complications such as thrombosis and bleeding should be shared when there is an absence of high-grade randomised data to guide clinical practice. This in-itself highlights the important need for further large-scale and quality international collaborative clinical trials in the area. With an ever-increasing plethora of TKI therapies becoming widely available in clinical use globally comes an equal need for close attention to adverse effects and treatment related complications. This can in many ways be better captured with improved access and input from multiple sites into global registries along with stringent reporting of adverse outcomes to overseeing authorities and government bodies approving therapies in their respective countries.


Comments (0)