
Remember me

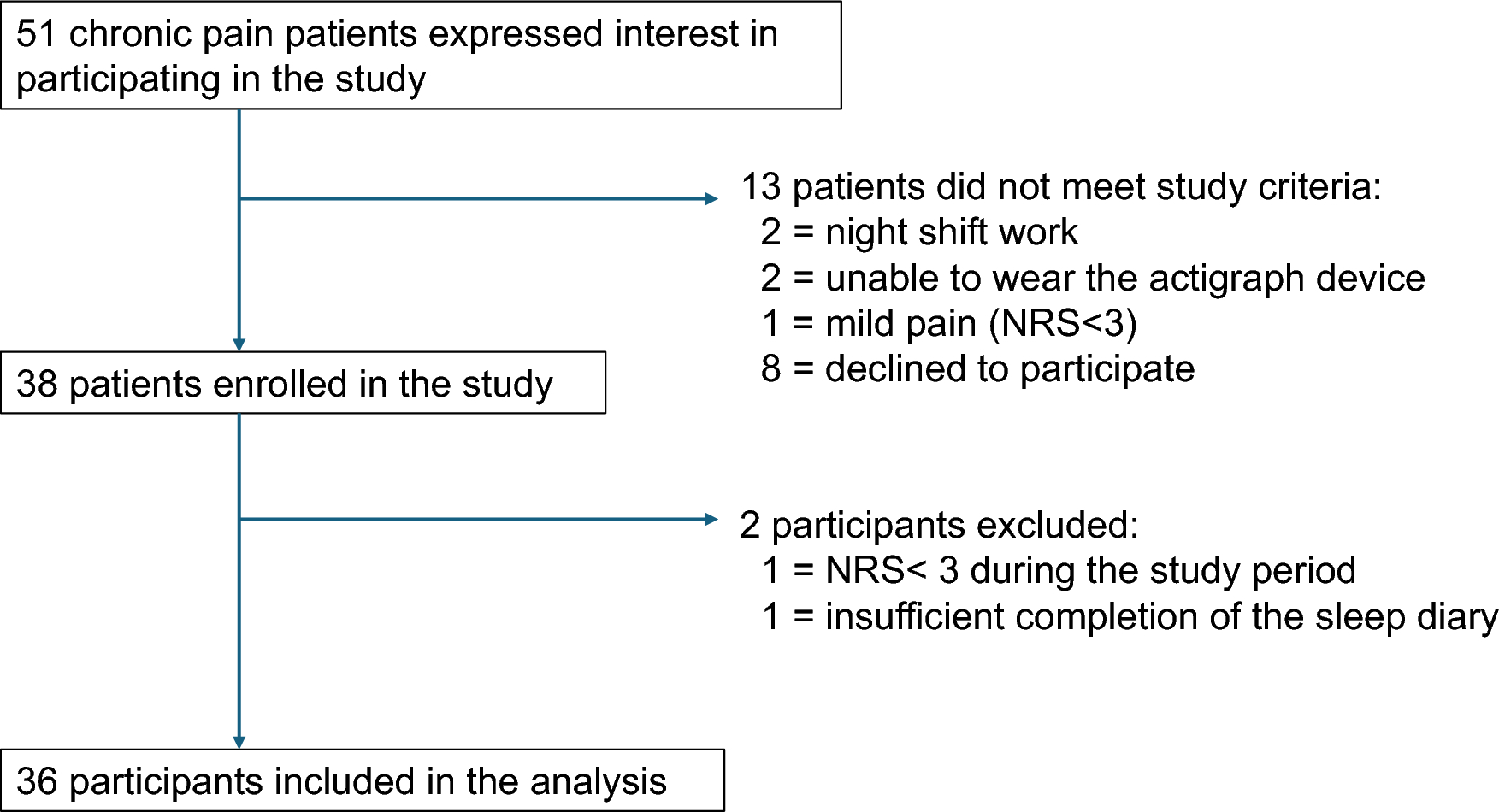

Eligible patients with chronic pain were recruited from outpatients attending the pain clinic at Yamaguchi University Hospital.
Inclusion criteria were as follows:
Age ≥ 18 years
Pain at the same site lasting ≥ 3 months
Pain intensity of ≥ 3 on the numerical rating scale (NRS) at the time of consent
Able to complete a medical questionnaire and sleep diary
Exclusion criteria were as follows:
Cancer pain
Psychiatric disorder with an obvious impact on pain and sleep (e.g., severe depression)
Working night shifts
Unable to wear an actigraph for long periods of time (e.g., due to working in an environment with strict hygiene standards or in construction)
No diseases or past treatments were set as exclusion criteria.
This study was approved by the Research Ethics Committee of Yamaguchi University Hospital.
Informed consent was obtained from all individual participants included in the study.
ProcedureParticipants completed a self-reported questionnaire about their pain, mental health (e.g., anxiety and depression), QOL, and sleep. After that, an actigraph (wGT3X-BT, ActiGraph, LLC; Pensacola, FL) was put on the non-dominant wrist of all participants. Participants were given written and verbal instructions explaining how to complete a sleep diary to self-evaluate their sleep for 8 consecutive days and how to use the actigraph. They were instructed to wear the actigraph at all times, except when bathing or showering, and to maintain their normal daily rhythm and sleeping/waking habits for the duration of the study. Participants were given a stamped mailing envelope to return the sleep diary and actigraph at the end of the study period. They were provided contact information for the institution conducting the study so that they could ask questions at any time during the study.
Participant assessmentSelf-reported questionnairesAt the time of enrollment, all participants completed a self-report questionnaire that included the following question items: basic clinical information (age, sex, diagnosis, disease duration); maximum, minimum, and average pain intensity within the past 24 h (NRS); Pain Catastrophizing Scale; Hospital Anxiety and Depression Scale; Athens Insomnia Scale; PainDETECT; and EuroQoL 5-Dimension.
The NRS is widely used to measure subjective sensations such as pain on a scale of 0 to 10. For pain intensity, participants self-rated their pain on an 11-point scale from 0 (no pain) to 10 (worst pain imaginable).
Daily subjective sleep assessment: sleep diary reportsThe sleep diary included the following items, and participants were instructed to make entries before sleep and after waking (Fig. 1). Before sleep: activities done during the day (e.g., eating, working, going out); and pain before sleep (NRS). After waking: bedtime, wakeup time, quality of sleep (NRS), and pain after sleep (NRS).
Fig. 1
Participants rated quality of sleep (NRS) on a scale from 0 (unsatisfactory) to 10 (satisfactory). Time in bed was defined as the time from bedtime to wakeup time. They recorded subjective ratings in the sleep diary for 8 days, from Day 1 to Day 8. However, to give participants time to get used to the actigraph, and to ensure that results reflected a weekly routine, only 7 days of data (from Day 2 to Day 8) were included in the analysis.
Daily objective sleep assessment: actigraphyThe following were evaluated as objective sleep data (Fig. 1): total sleep time, sleep onset latency, wake time after sleep onset, and sleep efficiency. Sleep was evaluated objectively using an actigraph (wGT3X-BT, ActiGraph, LLC) for 8 consecutive nights. An actigraph is a lightweight electronic device worn on the wrist and is used to measure physical activity and sleep with a three-axis accelerometer. Using specialized software (ActiLife 6 Data Analysis Software) and the Cole-Kripke scoring algorithm, we analyzed locomotor activity data in 60-s epochs to determine whether participants were asleep or awake.
Objective sleep data from the actigraph were combined with bedtime and wakeup time data from the sleep diary, and sleep onset latency (min) was calculated as the time from bedtime to sleep onset. Wake time after sleep onset (min) was calculated as the duration of wake epochs that occurred between sleep onset and the last wakeup. Total sleep time (min) was calculated as the total time in bed that was classified as sleep. Sleep efficiency was calculated using the following formula:
$$}\;}\;\left( \% \right) = \left( } \right)/\left( } \right) \times 00$$
Daily pain measurementParticipants recorded pain intensity ratings in their sleep diary twice a day—once before bedtime and once after waking—for 8 consecutive days. The change in pain after sleep (Δpain) was defined as the difference between pain from before sleep to after sleep:
$$\Delta } = \left( } \right)\left( } \right)$$
A positive Δpain indicates a higher pain intensity after sleep than before sleep, whereas a negative Δpain indicates a lower pain intensity after sleep (Fig. 2).
Fig. 2
Sleep and pain assessments by actigraphy and sleep diaries. Daily objective sleep assessments were made using an actigraph (wGT3X-BT) for 8 days. Daily objective sleep assessments included total sleep time, sleep onset latency, and wake time after sleep onset. Daily subjective sleep assessments were self-recorded by participants in sleep diary reports. Daily subjective sleep assessments included bedtime, pain before sleep, wake time, quality of sleep, and pain after sleep
Relative pain before sleep was defined as pain intensity before sleep relative to the participant’s average pain intensity:
$$\left( } \right) = \left( } \right) - \left( } \right)$$
A positive relative pain before sleep indicates higher than average pain, whereas a negative result indicates lower than average pain.
Statistical analysisTo evaluate the impact of relative pain intensity before sleep on objective sleep data and subjective sleep assessments from that night, a mixed-effects model was used with objective sleep data (sleep efficiency, total sleep time, sleep onset latency, and wake time after sleep onset) and quality of sleep set as dependent variables, and relative pain before sleep as a fixed effect. To evaluate the impact of objective sleep data and subjective sleep assessments on changes in pain after sleep, a mixed-effects model was used with Δpain set as a dependent variable, and age, sex, objective sleep data (sleep efficiency, total sleep time, sleep onset latency, and wake time after sleep onset) and quality of sleep as fixed effects.
We accounted for inter-individual variability by including a patient identifier as a random effect in the mixed-effects model. This approach allowed us to capture overall trends while considering differences in baseline conditions and individual responses among patients. Specifically, the model incorporated repeated measurements for each patient, enabling us to appropriately handle the longitudinal data and account for intra-individual correlations.
JMP Pro 16 (SAS Institute Inc.; Cary, NC) was used for statistical analysis. Participant characteristics were summarized as means and standard deviations for continuous variables, and as frequencies and percentages for categorical variables. All statistical tests were two-sided, with a significance level of 0.05.
Comments (0)