
Remember me




Infected pancreatic necrosis (IPN) is a life-threatening complication of acute necrotizing pancreatitis with substantial morbidity and mortality (1). However, diagnosis of IPN is challenging since the symptoms of noninfectious systemic inflammation can mimic signs of infection (2,3). Fine-needle aspiration (FNA), which has been recognized as an effective approach for early diagnosis of IPN since the late 1980s (4,5), may help facilitate differentiating IPN-related symptoms from systemic inflammatory response syndrome (SIRS).
However, FNA is no longer recommended as a routine approach in the current guidelines due to its high false-negative rate and invasiveness (6–8). Conventionally, specimens obtained by FNA were subjected to microbiological culture, which takes a long time and is not sensitive enough in some clinical circumstances (9,10). Metagenomic next-generation sequencing (mNGS) is a new technology for parallel sequencing of all microbe nucleic acids in a specimen, with a broad spectrum, including bacteria, viruses, fungi, atypical pathogens, parasites, and even new microorganisms (11). The mNGS technique has been used in multiple infectious diseases, including pneumonia, bloodstream infection, and encephalitis, demonstrating high sensitivity and timeliness, and is less affected by the use of antibiotics (12,13). For gastrointestinal diseases, the application of mNGS widens the pathogen spectrum compared with culture-based microbiological tests for acute intra-abdominal infections (14). Our previous study found that mNGS assays of pancreatic drainages could broaden the range of identifiable infectious pathogens and provide a more timely diagnosis of IPN (15).
In this study, we hypothesized that the addition of mNGS to the standard FNA procedure could enable faster detection of causative pathogens with satisfactory accuracy. The results from mNGS assays may help clinical decision-making and facilitate tailored treatment in patients with IPN.
METHODS Study design and patientsThis is a prospective, single-arm feasibility study. The study was approved by the Ethics Committee of the Jinling Hospital (Nanjing, China; 2021NZKY-014-01) and was registered with the China Clinical Trials Registry (registration number: ChiCTR2100047244) before enrollment.
From June 2021 to March 2022, we screened consecutive patients with acute pancreatitis (AP) admitted to the Center of Severe Acute Pancreatitis (CSAP) at Jinling Hospital. Study inclusion criteria were (i) AP diagnosed according to the Revised Atlanta classification (16); (ii) presence of pancreatic necrosis confirmed by computed tomography (CT) scan; (iii) age older than 18 years; (iv) admission within 1 week from AP onset; (v) written informed consent was obtained. Patients who were pregnant or who had prior abdominal or retroperitoneal invasive procedures were excluded.
During the index hospitalization and within 5 weeks of the onset of abdominal pain, eligible patients who developed suspected IPN would be formally enrolled. Suspected IPN was diagnosed based on clinical manifestations of fever (temperature ≥38.5°C) accompanied by elevated inflammatory serum markers. The air bubble sign in the necrotic collection demonstrated on CT was considered proof of confirmatory IPN (17); thus, patients with this radiological feature were excluded. Two investigators (Z.T. and L.K.) are responsible for making the diagnosis. Patients would not be enrolled until a consensus was reached.
The study subjects were treated according to the International Association of Pancreatology/American Pancreatic Association guidelines, including adequate fluid resuscitation, early enteral nutrition, vasopressor titration, mechanical ventilation, renal replacement therapy, and delirium management.
The FNA procedureWithin 24 hours of suspicion of IPN, CT-guided FNA would be performed. The pancreatic drainage specimens were sent simultaneously for mNGS and microbial culture. If the initial sample was negative for both mNGS and culture and the suspicion of IPN continued, the FNA procedure would be repeated within 72 hours. Up to 2 FNA procedures were applied to each study subject.
An independent adjudication committee consisting of 3 experienced clinicians would review the mNGS and culture results to decide if a change to the treatment was necessary. The changes include discontinuation/application of antibiotics, narrowing or extending antibiotic coverage, and performing invasive procedures such as percutaneous catheter drainage (PCD) and open surgery. The committee also decided on the following treatment when the mNGS and culture results were inconsistent.
mNGS processThe mNGS process was performed as described previously (18). In short, total genomic DNA was extracted with a TIANGEN DP316 kit (TIANGEN, Beijing, China). DNA libraries were constructed through DNA fragmentation, end-repair, adapter ligation, and PCR amplification. The qualified libraries were finally sequenced on a Nextseq 550 platform (Illumina, San Diego, CA). The screened sequences were finally aligned with the NCBI microorganism genome database for pathogen identification (https://ftp.ncbi.nlm.nih.gov/genomes/refseq/). Before analysis, the principal investigators cross-checked the data to ensure the quality of the data.
The results were considered completely consistent when the pathogens identified by mNGS and culture were the same (either positive or negative). The result was partially consistent when pathogens identified by the 2 methods were partially identical. The results were considered different when pathogens identified by the 2 methods varied completely.
Study outcomesThe primary outcome of this study is the diagnostic performance of the FNA-mNGS approach. Confirmatory IPN within the following week of the index FNA procedure was set as the reference standard. IPN was confirmed when a positive microbial culture from pancreatic necrosis was obtained by catheter drainage and/or necrosectomy. Otherwise, sterile pancreatic necrosis would be defined. Since all the study subjects underwent an invasive procedure, bubble signs within the pancreatic necrosis were not considered proof of IPN. In patients undergoing repeated FNA procedures, if the mNGS results obtained from the 2 procedures are inconsistent, it was counted as positive. Secondary outcomes include a comparison of pathogens detected by culture and mNGS approach and the impact of mNGS on clinical decision making.
The impact of mNGS on clinical decision making was divided into 2 categories: effective information and redundant information. Effective information refers to those leading to a change in treatment. Redundant information means that mNGS results were deemed false or insignificant.
Historical control patientsPatients with suspected or confirmed IPN admitted between January 2017 and December 2020 who met the abovementioned eligibility criteria were included in the historical control group. The clinical and laboratory data for the historical controls were extracted from a web-based electronic database. According to the electronic hospital records, clinical data on the day when suspected/confirmed IPN was first mentioned was set as the baseline. Propensity score matching was applied for baseline imbalances.
Clinical outcomes were compared between the study patients and historical control patients. The outcome measures include in-hospital mortality, 28-day mortality, length of intensive care unit stay, length of hospital stay, new-onset organ failure, sepsis defined according to the SEPSIS 3.0 definitions (19), and local complications. The definitions of organ failure were based on a score of ≥2 in the Sequential Organ Failure Assessment (SOFA) scoring system (20). The local complication included gastrointestinal fistula or abdominal bleeding requiring invasive intervention. New-onset in this study was defined as events that occurred after the baseline day. The SIRS and SOFA scores within 14 days (days 1, 3, 5, 7, and 14) were also calculated.
Statistical analysisContinuous variables were expressed as the median and interquartile range (25%–75%). Categorical variables were expressed in terms of frequencies and percentages. Mann-Whitney U tests were used to assess differences in continuous variables between groups. χ2 tests or Fisher exact tests were used to compare the categorical variables between groups. The sensitivity, specificity, positive predictive value, and negative predictive value of the mNGS tests for the reference standard are presented in a 2 × 2 contingency table.
To adjust for baseline imbalances, propensity score matching was used. The propensity score was estimated using logistic regression. The log odds of the probability that a patient received FNA were modeled for potential confounders: age, sex, and organ failure (respiratory, renal, and cardiovascular system) defined above when IPN was suspected. Subjects were 1:2 matched by the estimated propensity score using nearest-neighbor matching with a caliper of 0.20 SD of the logit of the propensity score. The quality of matching was assessed by calculating the standardized mean difference (SMD) between selected variables, with an SMD of <0.10 reflecting good matching. All statistical analyses were performed using statistical software (IBM SPSS statistics 26.0). All tests were 2-tailed, and P values of <0.05 were inferred as significant.
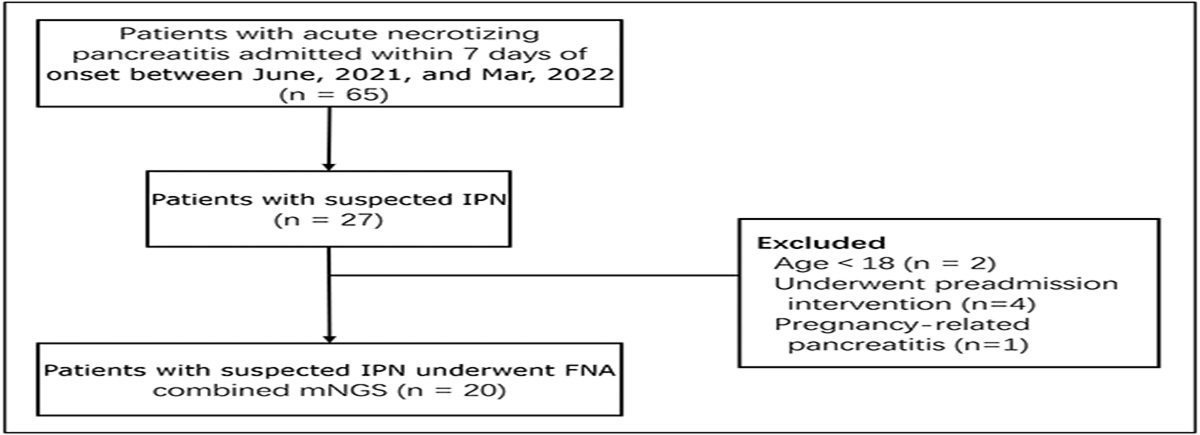
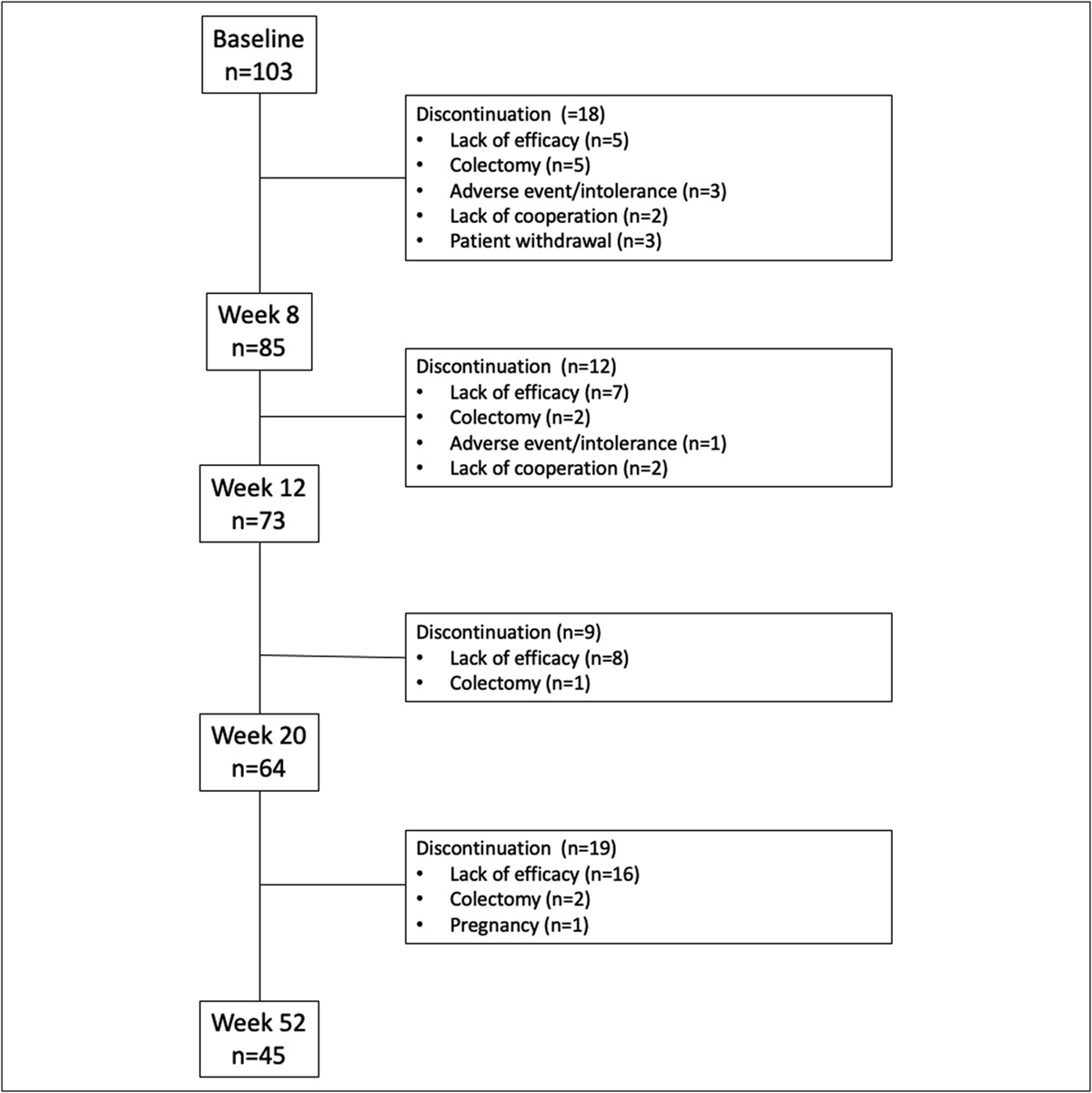
RESULTS Study participants and demographic characteristicsDuring the study period, 65 patients were screened and 27 potential participants with suspected IPN were assessed for eligibility. Seven were then excluded for reasons, and the remaining 20 patients were enrolled and underwent at least 1 FNA procedure (Figure 1).
 Figure 1.:
Figure 1.: Flowchart of participant inclusion in the trial. During the study period, 65 patients were screened and 20 patients were enrolled and underwent at least 1 FNA procedure. FNA, fine-needle aspiration; IPN, infected pancreatic necrosis.
The baseline characteristics of study patients are presented in Table 1. The median age of the study patients was 50 (34.5, 59.5) years, and 15 (75%) were male. A total of 18 patients were classified as having severe acute pancreatitis, and 14 patients had gallstones as the cause. The incidence of cardiovascular failure, renal failure, and respiratory failure was 25%, 40%, and 80% at enrollment, respectively.
Table 1. - Clinical characteristics of the study population Study cohort Age, yr 50 (34.5–59.5) Sex, male, n (%) 15 (75) Degree of severity, n (%) Moderately 2 (10.0) Severe 18 (90.0) Etiology, n (%) HTG 6 (30.0) Gallstone 14 (70.0) Cardiovascular failure, n (%) 5 (25.0) Renal failure, n (%) 8 (40.0) Respiratory failure, n (%) 16 (80.0) PCT, μg/L 3.91 (1.94–7.70) CRP, mg/L 187.2 (96.1–222.55) Leukocyte, ×109/L 13.42 (8.10–20.10) Neutrophils, ×109/L 11.06 (7.06–16.98) Time from onset to FNA, d 24.0 (19.5–29.5)Data are presented as n (%) or median (interquartile range). Propensity score matching was performed for these variables due to potential and/or significant effects on clinical outcomes.
CRP, C-reactive protein; FNA, fine-needle aspiration; HC, historical control; HTG, hypertriglyceridemia; PCT, procalcitonin.
The median time from symptom onset to the first FNA procedure was 24.0 (19.5–29.5) days. Eight microbe species were detected by mNGS, including 7 bacteria and 1 fungus (16 strains in total). Correspondingly, 9 microbial species were detected by culture, including 8 bacteria and 1 fungus (18 strains in total) (Figure 2a, c). There was no significant difference between mNGS and culture approaches in the positive rate (75% vs 70%, P = 0.723, Figure 2d).
 Figure 2.:
Figure 2.: Comparison of pathogens detected by metagenomic next-generation sequencing (mNGS) and culture. (a) Pathogens detected by the mNGS and culture method.s (b) Consistency between the mNGS and culture methods in the identification of the pathogen. (c) Comparison of the number of pathogens detected by the mNGS and culture methods. (d) The positive rates of pathogen detection by the mNGS and culture methods. (e) Time from sampling to reporting of the mNGS and culture methods.
The results of mNGS and culture were completely consistent in 70.0% (14/20), partially consistent in 10% (2/20), and different in 20.0% (4/20) (Figure 2b). In the 2 cases with partially consistent results, culture detected more pathogens than mNGS. For the 4 inconsistent cases, in 2 cases, the pathogens were detected by mNGS only; in 1 case by culture only; and in 1 case, the 2 methods detected different pathogens.
Diagnostic performance by FNA-mNGSA total of 16 patients had confirmatory IPN during the following week after the index FNA procedure. Overall, the accuracy of FNA-mNGS was 80.0%, with a sensitivity of 82.35%, specificity of 66.67%, positive predictive value of 93.3%, and negative predictive value of 40.0% (Figure 3). The mNGS assays showed a false-negative rate of 17.65% (3/17) and false-positive rate of 33.33% (1/3). All 3 false-negative patients underwent PCD the following week after the FNA procedure and had pathogens detected by culture, including Klebsiella pneumonia (n = 2) and Acinetobacter baumannii (n = 1).
 Figure 3.:
Figure 3.: The diagnostic performance of mNGS. IPN, infected pancreatic necrosis; mNGS, metagenomic next-generation sequencing; NPV, negative predictive value; PPV, positive predictive value; SPN, sterile pancreatic necrosis.
Clinical decision making based on the results of mNGSThe median time from sampling to reporting was 43 (43–43 hours) for the mNGS approach and 120 (70–168 hours) for the culture approach(P < 0.001) (Figure 2e).
All patients included in the study were given antibiotics at enrollment. The results of mNGS led to a change in treatment in 16 patients, including implementing PCD (n = 7), expanding antibiotic coverage (n = 2), a combination of PCD and expanding coverage (n = 4), narrowing antibiotic coverage (n = 1), and discontinuation of antibiotics (n = 2). In the remaining 4 cases, the results of mNGS were considered redundant information, including 3 false negatives (no action followed) and 1 case deemed as a noncausative pathogen. The details of the treatment decisions based on mNGS results for each patient are shown in Supplementary Table S1 (see Supplementary Digital Content 1, https://links.lww.com/CTG/B146).
Comparison with historical control patientsThe results of the PS matching are presented in Supplementary Figure S1 and Supplementary Table S2 (see Supplementary Digital Content 1, https://links.lww.com/CTG/B146). The study patients showed a higher PCT level compared with historical controls. After propensity score matching, the baseline characteristics were well balanced between the 2 groups, with the SMD being <0.10. Consequently, 20 study patients and 40 historical controls were analyzed. There were no significant differences in etiology, severity of AP, organ failure status, and serum inflammatory cytokines between matched study patients and historical control patients (see Supplementary Table S2, Supplementary Digital Content 1, https://links.lww.com/CTG/B146).
For clinical outcomes, there were no statistically significant differences in SIRS scores and SOFA scores between the 2 groups within 14 days of suspected IPN (Figure 4). In addition, there was no significant difference between the 2 groups regarding the length of hospital stay, length of intensive care unit stay, local complications, new-onset organ failure, and in-hospital mortality (Table 2).
 Figure 4.:
Figure 4.: SIRS score and SOFA score of the study patients and the historically controlled (HC) patients during the following 14 days since suspected infected pancreatic necrosis. (a) SIRS score of study patients and HC patients (P > 0.05). (b) SOFA score of study patients and HC patients (P > 0.05). SIRS, systemic inflammatory response syndrome; SOFA, Sequential Organ Failure Assessment.
Table 2. - Clinical outcomes of the matched study patients and historical control patients Study patients (n = 20) HC (n = 40) P value Infected pancreatic necrosis 17 (85.0) 30 (75.0) 0.513 Length of hospital stay, d 43.5 (35–74.25) 38 (31.25–71.25) 0.311 Length of ICU stay, d 33 (20.25–42.75) 23.52 (11.25–54.75) 0.689 In-hospital mortality 8 (40.0) 9 (22.5) 0.156 28-d mortality 4 (20.0) 4 (10.0) 0.422 Requiring open surgery 7 (35.0) 7 (17.5) 0.195 Local complication Gastrointestinal fistulas 3 (15.0) 7 (17.5) 1.000 Abdominal bleedinga 8 (40.0) 10 (25.0) 0.232 Sepsis 11 (55.0) 18 (45.0) 0.465 New-onset organ failure 10 (50.0) 12 (30) 0.130 New-onset cardiovascular failure 7 (35.0) 8 (20.0) 0.206 New-onset respiratory failure 3 (15.0) 4 (10.0) 0.570 New-onset renal failure 2 (10.0) 3 (7.5) 1.000HC, historical control; ICU, intensive care unit.
aAbdominal bleeding requiring invasive intervention.
In this study, we assessed the feasibility of the FNA-mNGS approach in patients with suspected IPN following acute necrotizing pancreatitis. Although the mNGS technique has an advantage in timeliness, adding mNGS to the standard FNA did not improve the diagnostic accuracy of conventional culture-based FNA procedures. The FNA-mNGS approach affected treatment in most of the study subjects, but no clinical benefits were observed compared with the historical controls.
Diagnosis of IPN is particularly difficult when it occurs early, and the FNA technique was developed for diagnosing such early infection (21,22). Usually, 2–3 weeks after the initial suspicion, the infection would be evident in many aspects such as clinical septic symptoms and laboratory findings, including but not limited to microbiological results. Since FNA was only applied during the first 24 hours of enrollment, it is possible infection developed after the initial FNA test if we extended to a wider time window. We set microbiological evidence within a week of the index FNA procedure as the gold standard to ensure the results can accurately reflect the infectious condition at the time of FNA.
The mNGS assays had a natural advantage since pathogens are detected by direct sequencing-extracted DNA from specimens, providing a broad microbial spectrum independent of a priori selection of target pathogens (23). In a recent study of 246 suspected pulmonary infection adults, mNGS assays of bronchoalveolar lavage fluid demonstrated an increased positive pathogen detection rate yield by approximately 25% over conventional tests (24). Another study on patients with focal infections found that mNGS was of satisfying diagnostic accuracy and detected 34 more causative microorganisms than culture (25). Inconsistent with previous studies, the FNA-mNGS approach did not detect more pathogens in this study. A possible explanation is that the spectrum of pathogens causing IPN is dominated by common microorganisms such as Enterobacteriaceae, Pseudomonadaceae, and Enterococcus (26,27), which can be easily identified by conventional methods.
The mNGS assays have shown excellent diagnostic performance in previous studies with specimens such as blood, pleural effusion and ascites, and cerebrospinal fluid (28–30). However, the FNA-mNGS approach showed unsatisfactory diagnostic performance in our study, and the spectrum of pathogens was similar between the mNGS and culture results. Notably, the false-negative rate, which is the biggest concern for FNA, was nearly 20% with the FNA-mNGS approach, similar to previous studies using culture-based FNA (17,31). The possible reason was that mNGS has an advantage in identifying fastidious and atypical microorganisms, but the predominantly pathogens of IPN can be recovered in standard culture conditions. Another reason may be that a small amount of fluid obtained by FNA could miss the pathogens in the collection.
Technically, the mNGS assays can significantly reduce the turnaround time for pathogen identification, which can potentially facilitate appropriate treatment decisions. A retrospective study showed that the mNGS approach and the following tailored antibiotics could reduce mortality in patients with severe pneumonia (32). On the contrary, our results showed that the mNGS-guided treatment did not improve clinical outcomes compared with the historical controls. The results are consistent with another study in 82 patients with suspected infection, showing that the mNGS assays had a positive impact in only 7.3% of the study subjects (33). The clinical futility of the FNA-mNGS approach in this study might be attributed to unsatisfactory diagnostic accuracy. Moreover, there is evidence showing that immediate or postponed invasive intervention did not affect clinical outcomes in patients with IPN (34); thus, timely intervention because of mNGS results may be just futile.
Several limitations need to be acknowledged. First, a relatively small sample size is a major limitation, which might influence the reliability of the results. Future large studies are needed to confirm or overturn our findings. Second, the single-arm design and the use of a historical control contain a high risk of bias. Finally, we used confirmatory IPN during the following week of the FNA procedure as the reference standard, but the infection can develop during that week, making the FNA results false negative.
In conclusion, the addition of the mNGS to the conventional FNA procedure did not enhance its diagnostic performance compared with the culture-based approach. Treatment adjustment can be implemented more timely with the mNGS results, but the clinical value needs to be studied in future parallel group trials.
CONFLICTS OF INTERESTGuarantor of the article: Lu Ke, PhD.
Specific author contributions: D.H.: data curation, writing—original draft. P.W. and Y.X.: investigation, data curation. S.X. and L.Y.: formal analysis, validation. W.L. and Z.T.: supervision, writing—review and edit. K.Q.: writing—review and editing. L.K.: conceptualization, funding acquisition. All authors contributed to the article and approved the submitted version.
Financial support: This work was supported by the grants from the National Nature Science Foundation of China (No. 82070665).
Potential competing interests: None to report.
Ethical approval: The study was approved by The Ethics Committee of the Jinling Hospital (Nanjing, China; 2021NZKY-014-01).
Data availability statement: The datasets are available from corresponding author on reasonable request.
Study Highlights
WHAT IS KNOWN ✓ Infected pancreatic necrosis (IPN) is a highly morbid complication of acute necrotizing pancreatitis. ✓ Fine-needle aspiration (FNA) is no longer recommended for the diagnosis of IPN. ✓ Metagenomic next-generation sequencing (mNGS) is a valuable tool for identifying potential pathogens. WHAT IS NEW HERE ✓ The addition of mNGS to standard FNA has comparable diagnostic accuracy with culture-based FNA. ✓ The FNA-mNGS approach may not be associated with improved clinical outcomes. REFERENCES 1. Forsmark CE, Vege SS, Wilcox CM. Acute pancreatitis. N Engl J Med 2016;375(20):1972–81. 2. Gukovskaya A, Gukovsky I, Algül H, et al. Autophagy, inflammation, and immune dysfunction in the pathogenesis of pancreatitis. Gastroenterology 2017;153(5):1212–26. 3. Huang D, Lu Z, Li Q, et al. A risk score for predicting the necessity of surgical necrosectomy in the treatment of infected necrotizing pancreatitis. J Gastrointest Surg 2023;27(10):2145–54. 4. Gerzof SG, Banks PA, Robbins AH, et al. Early diagnosis of pancreatic infection by computed tomography-guided aspiration. Gastroenterology 1987;93(6):1315–20. 5. Banks PA. Pro: Computerized tomographic fine needle aspiration (CT-FNA) is valuable in the management of infected pancreatic necrosis. Am J Gastroenterol 2005;100(11):2371–2. 6. Banks PA, Gerzof SG, Langevin RE, et al. CT-guided aspiration of suspected pancreatic infection: Bacteriology and clinical outcome. Int J Pancreatol 1995;18(3):265–70. 7. Working Group IAPAPAAPG. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013;13(4 Suppl 2):e1–15. 8. Baron TH, DiMaio CJ, Wang AY, et al. American Gastroenterological Association clinical practice update: Management of pancreatic necrosis. Gastroenterology. 2020;158(1):67–75.e61. 9. Geng S, Mei Q, Zhu C, et al. Metagenomic next-generation sequencing technology for detection of pathogens in blood of critically ill patients. Int J Infect Dis 2021;103:81–7. 10. Duan H, Li X, Mei A, et al. The diagnostic value of metagenomic next-generation sequencing in infectious diseases. BMC Infect Dis 2021;21(1):62. 11. Chiu C, Miller S. Clinical metagenomics. Nat Rev Genet 2019;20(6):341–55. 12. Simner P, Miller S, Carroll K. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis 2018;66(5):778–88. 13. Shen H, Liu T, Shen M, et al. Utilizing metagenomic next-generation sequencing for diagnosis and lung microbiome probing of pediatric pneumonia through bronchoalveolar lavage fluid in pediatric intensive care unit: Results from a large real-world cohort. Front Cell Infect Microbiol 2023;13:1200806. 14. Mao JY, Li DK, Zhang D, et al. Utility of paired plasma and drainage fluid mNGS in diagnosing acute intra-abdominal infections with sepsis. BMC Infect Dis 2024;24(1):409. 15. Hong D, Wang P, Zhang J, et al. Plasma metagenomic next-generation sequencing of microbial cell-free DNA detects pathogens in patients with suspected infected pancreatic necrosis. BMC Infect Dis 2022;22(1):675. 16. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013;62(1):102–11. 17. van Baal M, Bollen T, Bakker O, et al. The role of routine fine-needle aspiration in the diagnosis of infected necrotizing pancreatitis. Surgery 2014;155(3):442–8. 18. Hong D, Wang P, Chen Y, et al. Detection of potential pathogen in pancreatic fluid aspiration with metagenomic next-generation sequencing in patients with suspected infected pancreatic necrosis. Dig Liver Dis 2023;55(2):243–8. 19. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801–10. 20. Vincent JL, Moreno R, Takala J, et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996;22(7):707–10. 21. van Grinsven J, van Brunschot S, Bakker OJ, et al. Diagnostic strategy and timing of intervention in infected necrotizing pancreatitis: An international expert survey and case vignette study. HPB (Oxford) 2016;18(1):49–56. 22. Büchler MW, Gloor B, Müller CA, et al. Acute necrotizing pancreatitis: Treatment strategy according to the status of infection. Ann Surg 2000;232(5):619–26. 23. Han D, Li Z, Li R, et al. mNGS in clinical microbiology laboratories: on the road to maturity. Crit Rev Microbiol 2019;45(5–6):668–85. 24. Jin X, Li J, Shao M, et al. Improving suspected pulmonary infection diagnosis by bronchoalveolar lavage fluid metagenomic next-generation sequencing: A multicenter retrospective study. Microbiol Spectr 2022;10(4):e0247321. 25. Zhang HC, Ai JW, Cui P, et al. Incremental value of metagenomic next generation sequencing for the diagnosis of suspected focal infection in adults. J Infect 2019;79(5):419–25. 26. Wu D, Ding J, Jia Y, et al. Predictors of mortality in acute pancreatitis complicated with multidrug-resistant Klebsiella pneumoniae infection. BMC Infect Dis 2021;21(1):977. 27. Li X, Li L, Liu L, et al. Risk factors of multidrug resistant pathogens induced infection in severe acute pancreatitis. Shock 2020;53(3):293–8. 28. Kanaujia R, Biswal M, Angrup A, et al. Diagnostic accuracy of the metagenomic next-generation sequencing (mNGS) for detection of bacterial meningoencephalitis: A systematic review and meta-analysis. Eur J Clin Microbiol Infect Dis 2022;41(6):881–91. 29. Sun L, Zhang S, Yang Z, et al. Clinical application and influencing factor analysis of metagenomic next-generation sequencing (mNGS) in ICU patients with sepsis. Front Cell Infect Microbiol 2022;12:905132. 30. Chen H, Zhang Y, Zheng J, et al. Application of mNGS in the etiological diagnosis of thoracic and abdominal infection in patients with end-stage liver disease. Front Cell Infect Microbiol 2021;11:741220. 31. Rodriguez JR, Razo AO, Targarona J, et al. Debridement and closed packing for sterile or infected necrotizing pancreatitis: Insights into indications and outcomes in 167 patients. Ann Surg 2008;247(2):294–9. 32. Xie Y, Du J, Jin W, et al. Next generation sequencing for diagnosis of severe pneumonia: China, 2010–2018. J Infect 2019;78(2):158–69. 33. Hogan CA, Yang S, Garner OB, et al. Clinical impact of metagenomic next-generation sequencing of plasma cell-free DNA for the diagnosis of infectious diseases: A multicenter retrospective cohort study. Clin Infect Dis 2021;72(2):239–45. 34. Boxhoorn L, van Dijk S, van Grinsven J, et al. Immediate versus postponed intervention for infected necrotizing pancreatitis. N Engl J Med 2021;385(15):1372–81.
Comments (0)