
Remember me




Pancreatic cancer has historically had among the worst prognosis of all types of cancer, with dismal 5-year survival rates of 3% in the mid-1970s, rivalling the survival rates of liver/intrahepatic bile duct and esophageal cancer. Since then, the most up-to-date Surveillance, Epidemiology, and End Results data from 2012 to 2018 reflect a substantial improvement of esophageal and liver/intrahepatic bile duct 5-year survival rates to 21%, while pancreas cancer survival rates have improved only to 12% over the same time period, making it the deadliest type of cancer by site (1).
Pancreatic ductal adenocarcinoma (PDAC) is by far the most common subtype of pancreatic cancer, making up greater than 90% of all pancreatic cancer cases. Ascites involves the accumulation of fluid in the abdomen and can arise from both cancer-related and non-oncologic etiologies such as cirrhosis. Ascites in patients with gastrointestinal malignancy is relatively understudied compared with ascites in ovarian cancer, despite having a prevalence of up to 15% (2,3). Malignant ascites has been associated with poor prognosis in patients with cancer especially those with nonovarian cancer, although data on malignant ascites in patients with PDAC remain limited (2,4–10). Current standard of care focuses on the palliation of symptoms with (oftentimes serial) large volume paracentesis, indwelling catheter placement, shunts, intraperitoneal chemotherapy or systemic cancer therapy, and sometimes diuretics (2,6,8,11–14). Malignant ascites in pancreatic cancer is challenging to manage because there are no current guideline recommendations for ascites management in pancreatic cancer (13,15), but guidelines are desperately needed due to the high rate of complications associated with catheter placement and oftentimes poor outcomes in this group of patients despite current efforts in treatment (11,12).
The serum-ascites albumin gradient (SAAG) is of particular importance in the diagnosis of ascites in PDAC (6) because it may inform whether the etiology of the ascites is likely due to peritoneal carcinomatosis (low SAAG) or portal hypertension (high SAAG) which can determine prognosis and treatment strategies (16,17). Little is known about the relationship between portal hypertension and ascites in PDAC; potential causes of portal hypertension in this population include either those that are liver related (existing cirrhosis and Budd-Chiari syndrome) or nonliver related (lymphatic obstruction or portal vessel invasion by tumor, heart failure, or portal fibrosis) (6,7,16). Recent studies have reported evidence of portal hypertension–related ascites despite a lack of liver metastases or disease in a significant subset of patients with PDAC (2,16). A previous study of ascites in PDAC reported that 82% of the cohort had high SAAG ascites, while only 18% had low SAAG, although only a small fraction of the total patients had their ascitic fluid analyzed in this study (2). In this group, diuretics have been observed to be inconsistently used at proper doses despite reports of clinical efficacy and being a first-line treatment consideration (16,18). To the best of our knowledge, there are no clinical studies of diuretics in pancreatic cancer–associated ascites, and practicing oncologists rely on empirical therapy or guidelines for ascites due to cirrhosis (6,16,19).
We performed a comprehensive analysis of clinical and biological data in our institutional biobank to describe the incidence, associated clinical factors, and outcomes of ascites in pancreatic cancer, the relationship between portal hypertension and malignant ascites, and the outcomes of supportive treatments chosen for ascites in PDAC.
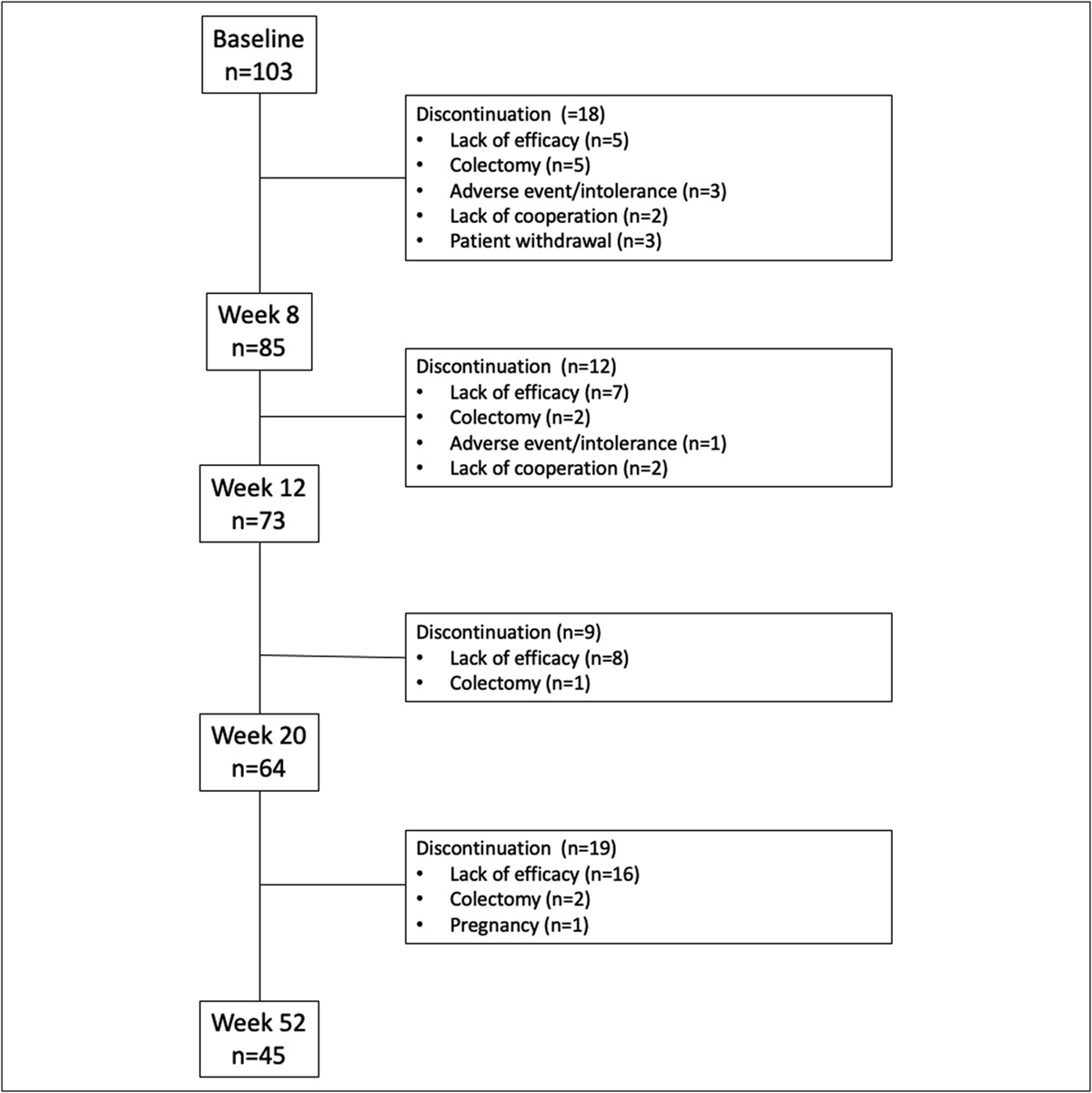
METHODSThe Gastrointestinal Biobank (“GI-Bank”) at Cedars-Sinai Medical Center collects patient specimens, associated clinical data, and self-reported questionnaires, without explicit inclusion or exclusion criteria. A total of 777 patients were prospectively and consecutively enrolled by practicing GI-oncologists in the GI-Bank by the time of analysis. Of these, 445 patients with complete data (meaning that all relevant demographics, clinical data, and outcomes had been entered into data consolidation software, without missing or unknown values) were included. All these patients had a pancreatic malignancy. Patients with pancreatic neuroendocrine tumors (n = 8) were excluded. Other histological subtypes, including adenosquamous (n = 7), acinar cell carcinoma (n = 1), and PDA with mucinous differentiation (n = 3), were considered sufficiently similar to PDAC (n = 426) to include in the analysis. Patients were not excluded based on any comorbidities i.e., a history of cirrhosis or congestive heart failure. Data were consolidated using a standard web application. All statistical analysis, except for univariate and multivariate Cox regression and logistic regression modeling, was conducted using Excel and using Datatab.net software tools. Univariate and multivariate Cox regression and logistic regression models were performed using R (version 4.1.2; R Core Team 2021).
RESULTSOf the 437 patients with PDAC, 182 (41.7%) developed ascites (Table 1). Ascitic fluid data were obtained in 104 patients; 88 (84.6%) had SAAG >1.1. Of patients with a low SAAG score <1.1 (n = 16, 15.4%), 7 (43.8%) had positive cytology whereas in patients with high SAAG >1.1 only 17 (19.3%) had positive cytology (Table 2). The estimated median survival from the diagnosis of ascites was 92 days (71–124) (Figure 1), and the median time to puncture was 7 days. The median time from first tap to death was 45 days (Table 2).
Table 1. - GI-Bank patient characteristics by ascites status Characteristic Total (N = 437) No ascites (N = 255) Ascites (N = 182) Age at diagnosis, median (IQR) 67 (61–74) 68 (62.5–76.5) 66 (58.25–72) Female, n (%) 208 (47.6) 120 (47.1) 89 (48.9) Race, n (%) White 297 (68.0) 187 (73.3) 110 (60.4) Black 31 (7.1) 16 (6.3) 15 (8.2) Asian 55 (12.6) 30 (11.8) 25 (13.7) Hispanic 45 (10.3) 20 (7.8) 25 (13.7) Other 9 (2.06) 2 (0.8) 7 (3.8)IQR, interquartile range.
SAAG, serum-ascites albumin gradient.
 Figure 1.:
Figure 1.: Survival after diagnosis of ascites. Kaplan-Meier estimates of survival in patients with pancreatic ductal adenocarcinoma after diagnosis of ascites. Estimated median survival 92 days (95% confidence interval 71–124).
To elucidate the association between potential risk factors in the patient history and development of ascites, logistic regression was performed. In univariate analysis, both the presence of metastasis to the peritoneum (defined by the presence of initial peritoneal metastases or recurrence to the peritoneum) and a history of ≥1 form of chemotherapy were significantly associated with ascites (Table 3), and this relationship remained significant in multivariate analysis (P = 0.011 for peritoneal metastases, P < 0.001 for a history of ≥1 form of chemotherapy) (Table 4). Metastasis to the liver, tumor resectability status, history of radiation or surgery, and SMAD4 mutation status were all not significantly associated with development of ascites (Table 3).
Table 3. - Univariate logistic regression of the outcome ascites Characteristic N OR 95% CI P value Initial CA 19-9 level 384 1.00 1.00–1.00 0.75 Resectability 436 0.17 Resectable — — Borderline resectable 2.09 1.08–4.08 Locally advanced 1.37 0.79–2.39 Metastatic 1.46 0.88–2.45 Initial metastasis site liver 437 0.54 No initial liver mets — — Initial liver mets 0.88 0.57–1.33 Initial metastasis site peritoneum 437 0.057 No initial peritoneal mets — — Initial peritoneal mets 2.28 0.98–5.58 Radiation history 437 0.69 No radiation — — At least 1 form of radiation 0.92 0.60–1.39 Chemotherapy history 437 <0.001 No chemotherapy — — At least 1 form of chemotherapy 5.82 2.44–17.2 Surgical history 437 0.37 Tumor not resected — — Tumor resected 0.83 0.55–1.25 smad4 genotype 437 0.15 WT — — SMAD4 mutation 0.51 0.18–1.27 Site of recurrence liver 437 0.84 No recurrence to liver — — Liver recurrence 1.04 0.69–1.57 Site of recurrence peritoneum 437 0.056 No peritoneal recurrence — — Peritoneal recurrence 2.38 0.98–6.12 Liver metastasis 437 0.78 No — — Yes 1.06 0.72–1.55 Peritonealmetastasis 437 0.00 5 No — — Yes 2.49 1.31–4.88The bold entries are variables that were found to be independently associated with the outcome ascites.
CI, confidence interval; OR, odds ratio; WT, wild-type.
CI, confidence interval; OR, odds ratio; WT, wild-type.
Patients were treated with either diuretics only (n = 69, 38.1%), PleurX catheter only (n = 20, 11.1%), both (n = 21, 11.6%), or neither (n = 71, 39.2%). Estimated median survival from the date of ascites diagnosis was highest in the group of patients who received both diuretics and PleurX (133 days [81–340]), followed by diuretics only (110 days [70–164]). Patients who received PleurX only had the lowest survival (54 days [42–264]) (Figure 2a–d).
 Figure 2.:
Figure 2.: Survival by treatment received. (a) Treated with diuretics, N = 69, censored N = 15 (21.7%). Estimated median survival 110 days (95% CI 70–164). (b) Treated with PleurX, N = 21, censored N = 0 (0%). Estimated median survival 54 days (95% CI 42–264). (c) Treated with both diuretics and PleurX, N = 21, censored N = 1 (4.8%). Estimated median survival 133 days (95% CI 81–340). (d) Treated with neither diuretics nor PleurX, N = 71, Censored N = 9 (12.7%). Estimated median survival 82 days (95% CI 48–116). CI, confidence interval.
Overall survival (OS) between ascites and nonascites groups were significantly different by log-rank test (P = 0.001), and the estimated median OS was 473 days (95% confidence interval [CI] 407–537) in patients with ascites vs 573 days (95% CI 473–681) in nonascites patients (Figure 3). In multivariate Cox regression analysis, positive ascites status, presence of liver metastases, an Eastern Cooperative Oncology Group of 3 or higher, and borderline or nonresectable primary tumor status were significantly associated with decreased survival. Ascites status carried a hazard ratio (HR) of 1.35 (1.04–1.76). Liver metastases (defined by the presence of initial liver metastases or recurrence to the liver) carried a HR of 1.56 (1.17–2.07). Compared with fully resectable primary tumors, borderline resectable status carried a HR of 1.87 (1.22–2.87), locally advanced HR 3.23 (2.21–4.73), and metastatic HR 2.94 (1.99–4.34). Compared with patients with an Eastern Cooperative Oncology Group of 0, scores of 1 and 2 were not significantly associated with decreased survival but higher scores of 3 and 4 were (HR 3.38 and HR 5.35, respectively) (Table 5). The presence of peritoneal metastases was not associated with significantly decreased survival in univariate analysis (Table 6).
 Figure 3.:
Figure 3.: Overall survival by ascites status. Kaplan-Meier estimates of survival in patients with PDAC with and without ascites. The estimated median overall survival for the ascites group was 473 days (95% CI 407–537). The estimated median overall survival for the nonascites group was 573 days (95% CI 473–681). CI, confidence interval; PDAC, pancreatic ductal adenocarcinoma.
Table 5. - Cox regression model: Multivariate analysis Characteristic HR 95% CI P value Age 1.02 1.00–1.03 0.006 Race White — — Other 2.38 1.01–5.56 0.046 African American 0.71 0.43–1.19 0.2 Asian 1.03 0.72–1.49 0.9 Hispanic 0.94 0.62–1.41 0.8 ECOG 0 — — 1 0.98 0.67–1.44 >0.9 2 1.53 0.88–2.66 0.13 3 3.38 1.78–6.42 <0.001 4 5.35 1.54–18.6 0.008 Resectability Resectable — — Borderline resectable 1.87 1.22–2.87 0.004 Locally advanced 3.23 2.21–4.73 <0.001 Metastatic 2.94 1.99–4.34 <0.001 Ascites No ascites — — Ascites 1.35 1.04–1.76 0.023 Liver metastasis No — — Yes 1.56 1.17–2.07 0.002CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio.
Risk factors with P > 0.2 (sex and tumor location) were excluded from the multivariate model. Model without perit_mets and rad_hx (both had P values >0.2).
CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio.
This prospective cohort analysis is the largest to date of patients with PDAC with respect to ascites. Ascites was a poor prognostic factor in our patients with PDAC, with median survival of 92 days after diagnosis of ascites. This translated into a decrease in median OS of 100 days between patients with and without ascites. In Cox multivariate analysis, having ascites was associated with a HR of 1.37 and carried a statistically significant increased likelihood of death. The incidence of portal hypertension–associated ascites was nearly 80%, significantly higher than previously reported by some studies (16) and consistent with a recent analysis performed at Memorial Sloan Kettering Cancer Center (2).
Despite ascites being an important prognostic factor for patients with PDAC, little is known about its etiology in pancreas cancer. We attempted to address the question of why ascites develops in some patients with PDAC but not others. In multivariate logistic regression analysis, metastasis to the peritoneum was significantly associated with ascites, which likely represents the subset of patients with peritoneal carcinomatosis and ascites, a well-known cause of malignant ascites. However, this subset only represented a minor subset of our study population, in which nearly 80% of patients had a high SAAG score (indicating portal hypertension as the primary cause of ascites) and low rates (<25%) of positive cytology. In patients with PDAC in this data set, portal hypertension, rather than peritoneal carcinomatosis, was the leading cause of ascites, although the exact mechanism leading to it remains unclear.
Liver metastases have been reported to both correlate with poor OS and development of malignant ascites in patients with PDAC (
Comments (0)