
Remember me




Functional bowel disorders (FBDs) are common disorders of the gut-brain interaction characterized by abdominal pain and/or discomfort, bloating, and altered bowel habit in the absence of anatomic or physiologic abnormalities (1). Subtypes of FBD include irritable bowel syndrome (IBS), functional constipation (FC), functional bloating (FB), functional diarrhea (FDr), and unspecified FBD (U-FBD) according to Rome III criteria (2). Previous studies spanning diverse population and healthcare settings reported high prevalence of FBD, ranging from 29% to 46% (3–5). Medical treatment of FBD is limited. Recurrent and chronic gastrointestinal (GI) symptoms result in compromised quality of life, loss of work productivity, and substantial utilization of healthcare resources (6–8).
Long-term studies examining the natural history of FBD including the evolution of symptoms and health outcomes are sparse and have been examined mainly in Western population. Two population-based studies performed in the United States and the United Kingdom demonstrated that prevalence of FBD appeared stable over time but change in symptoms were frequent (9–11). Furthermore, some studies have demonstrated increased risk of organic disease such as inflammatory bowel disease (IBD) or colorectal cancer among patients with FBD compared with those without FBD over time (12–15). Other studies have suggested that patients with FBD may have elevated risk of undergoing cholecystectomy compared with the general population given recurrent and chronicity of gastrointestinal (GI) symptoms leading to excessive medical examination (16,17). Finally, limited long-term population-based studies showed that individuals with FBD do not have elevated risk of mortality compared with the general population (18,19).
Variable prevalence of FBD across different geographic regions and healthcare settings have limited the generalizability of findings from a sparse number of available studies. Furthermore, natural history of FBD in Chinese population is undefined, and whether the results parallel findings in Western population are unknown. Few population-based studies evaluated health outcomes such as development of organic disease or need for abdominal/pelvic surgery during long-term follow-up. Psychological comorbidities including anxiety or depression have been reported to be linked with FBD (20). However, most of these cross-sectional studies did not allow for true causal associations to be assessed (21–23). Longitudinal studies performed in community settings examining the association of psychological factors with FBD are sparse. Limited studies, mainly in IBS and functional dyspepsia, demonstrated that dysfunction of the gut-brain pathway was a driver of GI symptoms (24,25). Instead of patients with IBS, we focused on a broader group of individuals with FBD for greater generalizability of findings. The aim of our study was to evaluate and compare the long-term natural history of individuals who meet criteria for FBD including symptoms, need for abdominal/pelvic surgery, development of GI organic disease, and mortality compared with those without FBD from a Chinese community. We also aimed to evaluate whether there may be a causal relationship between FBD and anxiety and/or depression by following a community-based cohort.
METHODS ParticipantsHangzhou is a major metropolitan city of 12.4 million inhabitants located in South-East China. The local population comprises mainly Han Chinese (99.8%), and the population is generally representative of the urban Chinese population comprising 92% Han ethnicity. Community inhabitants, 16–74 years of age, were selected by randomized sampling of residential address in 1 of 5 Hangzhou communities using local census published in January 2010. Individuals were stratified by age and sex. This stratified randomized cluster sampling of individuals was performed to obtain a representative sample of the local population. Community members were invited to attend a face-to-face interview to complete the questionnaires with the assistance of community health workers and medical students. Of the 2,115 individuals who had participated in the baseline random population community survey, 1,999 (95%) met the study criteria. Subsequently, 840 of 1,999 (42%) agreed to participate in future follow-up studies. Individuals who completed an extensive community-based survey on FBD in January 2010 and agreed to be recontacted for future research were eligible for this study. Individuals receiving treatment of organic diseases of the GI tract (eg, cancer, IBD, and peptic ulcer) and other diseases known to affect GI function (eg, diabetes) were excluded during completion of the baseline survey. Original cross-sectional study was independently conducted in 2010 by the same investigators to assess the prevalence and factors associated with FBD in a representative Chinese population (4). Baseline data including demographic data, smoking and alcohol consumption, symptoms of FBD using the Rome III questionnaire, and anxiety and depression scales were collected. This study was approved by the ethical committee of Sir Run Shaw Hospital (ClinicalTrials.gov Identifier: NCT01286597, approval date: August 23, 2008).
Individuals who agreed to participate in a long-term study were contacted via a telephone between September and December 2018 to complete a questionnaire to obtain data on the presence of FBD symptoms (Rome III criteria), psychological conditions, interval incidence of abdominal/pelvic surgery, interval incidence of organic disease, and survival. Primary end point was diagnosis meeting at least 1 FBD (IBS, FDr, FB, FC, U-FBD) based on Rome III criteria. When multiple diagnostic criteria for FBD were met, patients were categorized using a hierarchical classification proposed by Rome III criteria that prioritize IBS over FDr or FC, IBS or FDr or FC over FB, and unspecific FBD when other criteria for FBD were not met (2). Secondary end points included interval incidence of organic disease (ie, IBD, GI, or liver cancer), abdominal and/or pelvic surgery, and death at the end of 9-year follow-up. Financial compensation of approximately 3$ was provided for the individuals who completed the telephone survey.
Survey questionnaireRome III Diagnostic Questionnaire designed by the Rome committee for FBD was used for this study (2). The FBD module can be downloaded from the Rome Foundation website (http://www.romecriteria.org/questionnaires). As per previous study, we adopted the standard Rome III questionnaire in the Chinese version through a routine process of translation and back translation (26). To ensure the consistency of diagnostic criteria and minimize reporting bias across time, Rome III questionnaire were uniformly adopted for both initial and follow-up surveys. Additional translated and validated questionnaires were used (27).
General: Demographic data of individuals (age, sex, education, job, family income, cigarette use, alcohol consumption) and medical history (ie, peptic ulcers, chronic diarrhea, and history of abdominal/pelvic surgery). Functional Bowel Disorder Questionnaire: The Part B Rome III Functional Bowel Disorder Questionnaire was used to diagnosis (2). Hospital Anxiety and Depression Scale: The Hospital Anxiety and Depression Scale questionnaire that includes standardized assessment of 14 items to evaluate anxiety (7 items with a maximum score of 21) and depression (7 items with a maximum score of 21) was used. Clinically significant anxiety or depression was defined by a score >11, respectively (28). DataBased on the data extracted from the questionnaire, individuals were categorized to those with or without FBD at baseline and at 9-year follow-up. Furthermore, individuals with FBD diagnosis was further categorized to 1 of 5 subgroups (IBS, FC, FB, FDr, and U-FBD). Results from the initial (2010) and final surveys (2018) were matched to categorize those with stable or had a change in diagnosis. The transition probabilities were calculated for each of the 6 symptom subgroups and demonstrated by a 7 × 7 table. Furthermore, individuals were categorized into 4 groups ([1] stable diagnosis of FBD, [2] change to a different FBD subtype, [3] resolution of FBD, or [4] new diagnosis of FBD) to evaluate the proportion of individual who had an interval change in diagnosis. Stability rates of FBD subtypes were defined as the proportion of individuals with FBD subtype at baseline survey who continued to meet Rome III criteria for the same subtype at 9-year follow-up.
StatisticsTo assess whether individuals successfully contacted by survey were representative of the baseline cohort, differences in demographic and clinical characteristics of individuals were evaluated by χ2 test for categorical variables and Student t test for continuous variables, respectively. Cross-sectional evaluation was performed to estimate the prevalence of FBD and the subtypes of those who completed the survey in 2 time periods. Change in diagnosis of FBD and health outcomes between the initial and follow-up surveys were compared by using the χ2 test. Logistic regression adjusting for age and sex was used in cross-sectional analyses both at baseline and at follow-up to analyze associations of FBD with anxiety and/or depression. Furthermore, among individuals who completed the follow-up survey, univariate analysis was performed to evaluate risk factors associated with two clinical end points, new-onset anxiety and/or depression and new-onset FBD symptoms. Risk factors, such as age, sex, education, job, family income, cigarette use, and alcohol consumption, which may be associated with clinical end points on univariate analysis (P value < 0.2), were evaluated by multivariate logistic regression to identify independent predictors of end points (2-sided P value < 0.05). Statistical analyses were conducted using SPSS (IBM, Armonk, NY; version 22). A two-tailed P value < 0.05 was considered statistically significant.
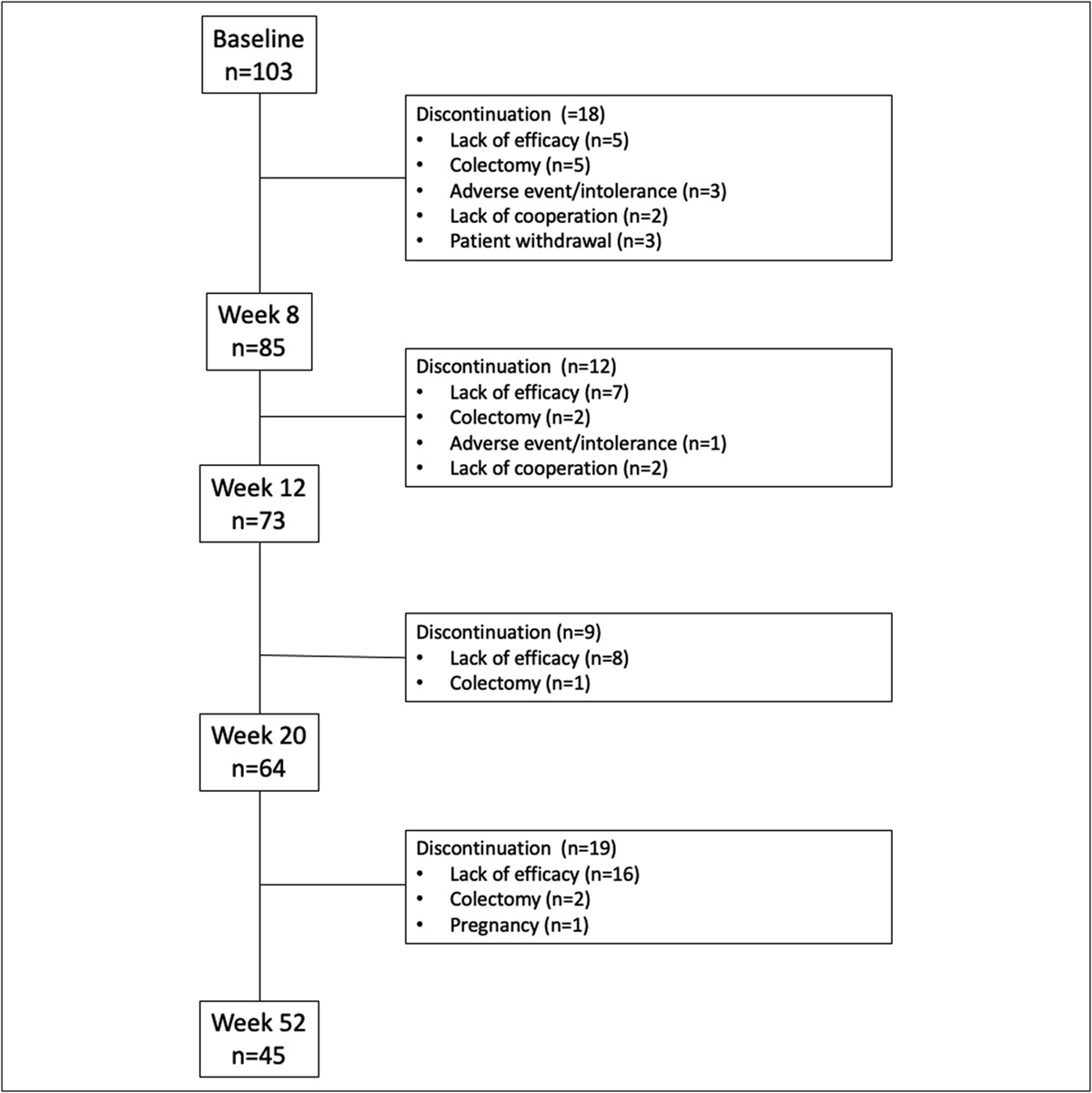
RESULTS SurveyOf the 1,999 individuals who had participated in the baseline random population community survey, 840 (42%) agreed to be recontacted for future follow-up research. No differences in age stratification, occupation type, average family income, cigarette smoking, alcohol, drinking use, and medical history were observed between the original survey cohort and individuals who agreed to participate in the follow-up (P > 0.05; Table 1). However, we found that more female patients agreed to participate in the follow-up survey (61% vs 50%, P < 0.05). Questionnaires were completed by telephone follow-up, and a total of 452 individuals completed the follow-up questionnaire, yielding a response rate of 54% (Figure 1). Six potential individuals were ineligible to complete the questionnaire due to death in 4 (hepatocellular carcinoma [HCC] in 2, lung cancer in 2) or Alzheimer dementia in 2. However, 4 patients were included in the analysis evaluating the secondary end point of death. Furthermore, 382 individuals were not able to be reached by phone.
Table 1. - Demographic data of the original survey and individuals who agreed to participate in the follow-up Variables Original survey cohort (N = 1,999) Follow-up cohort (N = 840) P value Age 0.23 <30 506 (25%) 194 (23%) 30–60 1189 (60%) 514 (61%) >60 304 (15%) 132 (16%) Sex 0.00 Male 1001 (50%) 326 (39%) Female 998 (50%) 514 (61%) Education 0.11 ≤High school 1253 (63%) 553 (66%) ≥College 746 (37%) 287 (34%) Job 0.21 Office work 351 (18%) 136 (16%) Physical work 767 (38%) 310 (37%) Housework 732 (37%) 347 (41%) Student 148 (7%) 47 (6%) Average family income (CNY) 0.15 <1000 200 (10%) 101 (12%) 1000–10,000 1728 (86%) 724 (86%) >10,000 71 (4%) 25 (2%) Cigarette smokinga 0.3 No 1498 (75%) 645 (77%) Yes 501 (25%) 195 (23%) Alcohol drinkingb 0.10 No 764 (38%) 349 (41%) Yes 1235 (62%) 491 (59%) Medical historyc 0.85 No 1597 (80%) 674 (80%) Yes 401 (20%) 166 (20%)CNY, Chinese Yuan.
aCigarette use (more than 1 cigarette per d).
bAlcohol consumption (more than 1 d per wk)
cMedical history including peptic ulcers, chronic diarrhea, and history of abdominal operation.
 Figure 1.:
Figure 1.: Flow diagram of the study selection process. FBD, functional bowel disorder.
Among the 840 individuals who agreed to be recontacted for follow-up research, participants who completed the follow-up survey had a higher educational level (38% vs 30%, P = 0.02), but no difference of age, sex, job type, average family income, cigarette smoking, alcohol, drinking use, and medical history were observed between the two groups (P > 0.05; Table 2). Furthermore, for the 452 of 840 individuals who completed the follow-up survey, no difference in age, sex, educational level, job type, average family income, cigarette use, alcohol consumption, and medical history were observed between the FBD and non-FBD groups (P > 0.05; Table 3).
Table 2. - Demographic data of responders and nonresponders Variables Responder (N = 452) Nonresponder (N = 388) P value Age 44.6 ± 15.3 44.4 ± 14.4 0.84 Sex 0.84 Male 174 (38%) 152 (39%) Female 278 (62%) 236 (61%) Education 0.02 ≤High school 281 (62%) 272 (70%) ≥College 171 (38%) 116 (30%) Job 0.11 Office work 86 (19%) 50 (13%) Physical work 161 (36%) 149 (38%) Housework 179 (39%) 168 (43%) Student 26 (6%) 21 (6%) Average family income (CNY) 0.21 <1000 46 (10%) 55 (14%) 1000–10,000 398 (88%) 326 (84%) >10,000 8 (2%) 7 (2%) Cigarette smokinga 0.26 No 354 (78%) 291 (75%) Yes 98 (22%) 97 (25%) Alcohol drinkingb 0.86 No 189 (42%) 160 (41%) Yes 263 (58%) 228 (67%) Medical historyc 0.91 No 362 (80%) 312 (80%) Yes 90 (20%) 76 (20%)CNY, Chinese Yuan.
aCigarette smoking (more than 1 cigarette per d).
bAlcohol drinking (more than 1 d per wk).
cMedical history including peptic ulcers, chronic diarrhea, and history of abdominal operation.
CNY, Chinese Yuan; FBD, functional bowel disorder.
aCigarette smoking (more than 1 cigarette per d).
bAlcohol drinking (more than 1 d per wk).
cMedical history including peptic ulcers, chronic diarrhea, and history of abdominal operation.
Of the 1,999 individuals who participated in the baseline survey, 840 (42%) consented but 452 (23%) completed the follow-up survey. The overall prevalence of FBD was 36.3% (95% confidence interval [CI] 32.6–40.0%) at enrollment and remained unchanged at 36.1% (95% CI 32.3–39.8%) at follow-up (P = 0.94) in the study population. The baseline prevalence of FBD among 840 individuals who consented to a follow-up study was similar (39.9%, 95% CI 36.6–43.2%; P = 0.21) to the baseline prevalence of the study population. Transition of symptom subgroups between the initial and final surveys was further analyzed based on the 452 individuals who had completed both the baseline and follow-up surveys. In the 9-year follow-up, 88 (54%) of 164 individuals diagnosed with FBD at the baseline survey continued to meet criteria for FBD including IBS in 16 (10%), FB in 8 (5%), FC in 26 (16%), FDr in 16 (10%), and U-FBD in 22 (13%). Conversely, 76 individuals (46%) with FBD at the baseline survey no longer met diagnostic criteria for FBD. Among FBD subtypes, stability rates were 15% (6 of 40) in FC, 5% (1 of 22) in FB, 14% (4 of 29) in FDr, 22% (8 of 36) in IBS, and 16% (6 of 37) in U-FBD (Figure 2). Of those 288 either asymptomatic or did not meet diagnostic criteria for FBD at baseline, 213 (74%) remained asymptomatic at follow-up while 75 (26%) reported symptoms met diagnostic criteria for FBD. Overall, 214 (47.3%) of 452 individuals who completed the 9-year follow-up survey had different diagnosis between the initial and follow-up surveys (Figure 2).
 Figure 2.:
Figure 2.: Transitions of symptom subgroups between the initial and final surveys (N = 452). FB, functional bloating; FBD, functional bowel disorder; FC, functional constipation; FDr, functional diarrhea; IBD, inflammatory bowel disease; IBS, irritable bowel syndrome; U-FBD, unspecified FBD.
Health outcomes at 9-year follow-upDuring the 9-year follow up, no individual developed new-onset IBD. Four patients in the FBD (rectal cancer in 1, HCC in 1) and non-FBD (gastric cancer in 1, HCC in 1) groups developed GI cancer. Among patients with FBD, rectal cancer and HCC were diagnosed at 72 and 60 months from enrollment, respectively. Among patients without FBD, gastric cancer and HCC were diagnosed at 48 and 72 months from enrollment, respectively.
A higher proportion of patients with FBD (17/164, 10.4% vs 10/288, 3.5%, P = 0.003) compared with non-FBD at baseline underwent abdominal and/or pelvic surgery over the 9-year period. Furthermore, more patients with FBD (16/164, 9.8% vs 9/288, 3.1%, P = 0.003) underwent non-cancer-related abdominal and/or pelvic surgery compared with those without FBD. Among individuals with FBD at the baseline survey, cholecystectomy was performed in 6 (3.7%), appendectomy in 2 (1.2%), gynecological surgery in 2 (1.2%), hemorrhoid surgery in 5 (3.0%), anal fistula surgery in 1 (0.6%), and rectal cancer surgery in 1 (0.6%). Among individuals without FBD at the baseline survey, cholecystectomy was performed in 3 (1.0%), appendectomy in 2 (0.7%), gynecological surgery in 1 (0.4%), hemorrhoid surgery in 1 (0.4%), anal fistula surgery in 1 (0.4%), inguinal hernia surgery in 1 (0.4%), and gastric cancer resection in 1 (0.4%) at follow-up.
Finally, during follow-up, 1 (0.6%) of 165 in individuals with FBD and 3 (1.0%) of 291 without FBD died without a significant difference (P = 0.64). Among those with FBD at baseline, the cause of death was HCC. Among those without FBD at baseline, the causes of death included HCC and lung cancer.
FBD at baseline is linked to new-onset anxiety and/or depressionDiagnosis of FBD was associated with anxiety and/or depression at the initial survey (AOR = 1.7, 95% CI 1.7–2.7, P = 0.02) and follow-up (AOR = 8.0, 95% CI 3.2–20.0, P < 0.001). Diagnosis of FBD at baseline was associated with new-onset anxiety and/or depression at follow-up (AOR = 3.2, 95% CI 1.2–8.3, P = 0.01) among the 297 individuals without anxiety and/or depression at the initial survey (Table 4). When analyzing anxiety and depression as a separate psychologic comorbidity, baseline diagnosis of FBD was not associated with new-onset anxiety (AOR = 1.7, 95% CI 0.4–8.2, P = 0.3) or depression (AOR = 3.9, 95% CI 0.7–22.0, P = 0.1) at follow-up. Among 288 individuals without FBD at baseline, anxiety and/or depression at baseline was not associated with increased likelihood of new-onset FBD at follow-up (Table 5). Anxiety and/or depression at follow-up (AOR = 5.86, 95% CI 1.7–20.1, P = 0.005) was associated with increased likelihood of new-onset FBD at follow-up.
Table 4. - Univariate and multivariate analyses for anxiety and depression new onset at 9-yr follow-up (N = 297) Variable Unadjusted OR P value Adjusted OR 95% CI P value Age 1.01 0.59 — Sex Male 1.00 — Female 1.11 0.84 — Education ≤High school 1.00 — ≥College 0.98 0.96 — Job Office work 1.00 — Physical work 0.8 0.71 — Housework 0.54 0.33 — Student 0.76 0.81 — Average family income (CNY) <1000 1.00 1000∼ 2.03 0.50 — 5000∼ 0.00 0.99 — ≥10,000 0.00 0.99 — Cigarette smokinga No 1.00 1.00 Yes 0.20 0.12 0.25 0.03–1.92 0.18 Alcohol drinkingb No 1.00 — Yes 1.08 0.88 — FBD diagnosis at baseline No 1.00 1.00 Yes 3.59 0.008 3.20 1.23–8.32 0.017CI, confidence interval; CNY, Chinese Yuan; FBD, functional bowel disorder; OR, odds ratio.
aCigarette use (more than 1 cigarette per d).
bAlcohol consumption (more than 1 d per wk).
Comments (0)