This is the first prospective prevalence study of potential prescribing cascade prevalence in hospitalised multimorbid older adults exposed to polypharmacy. It demonstrates that prescribing cascades are substantially prevalent in this population to a clinically significant degree, particularly among those who experience hyperpolypharmacy. The analysis of drug pairs where drug A was prescribed followed by drug B compared with the reverse order suggests that the suspected prescribing cascades identified in this study are likely to be clinically valid. Although the more frequent prescribing in the sequence drug A → drug B does not definitively confirm their status as prescribing cascades, it supports the hypothesis that the potential prescribing cascades identified in this study are true prescribing cascades. This is important, as true prescribing cascades can have serious adverse consequences for patient safety and healthcare outcomes [5].
As ageing demographic trends intensify as a global phenomenon, the prevalence of multimorbidity is increasing in tandem, resulting in ever increasing levels of polypharmacy and hyperpolypharmacy [21,22,23]. As older people are prescribed more medications, their risk of experiencing inappropriate prescribing (IP) in general also rises [13, 24]. The present study aligns with this observed association, confirming that potential prescribing cascades as another manifestation of IP are associated with a higher number of prescribed medications [25].
While the management of patients with complex multimorbidity and associated polypharmacy has traditionally been the responsibility of general practitioners and geriatricians, the responsibility for medication management will increasingly extend to all physicians dealing with multimorbid older people in their own areas of clinical practice. In the present study, 84% (n = 326) of patients were under the care of physicians who were not geriatricians, i.e. specialists without specific training in age-related multimorbidity and associated complex polypharmacy. Without the necessary training and experience in geriatric medicine, these physicians may struggle to recognise prescribing cascades, as was evident in the present study where very little curtailment of potential cascades was evident between admission and discharge, possibly related to lack of recognition of potential cascades. This challenge is compounded by the fact that ADEs in older adults with multimorbidity are more challenging to recognise and can often present with non-specific symptoms, such as new-onset confusion, gastrointestinal upset and dizziness [4, 26, 27].
A recent systematic review by Adrien et al. assessed recommendations for addressing prescribing cascades [10]. Fewer than half of the studies included in the review provided specific guidance on reversing inappropriate prescribing cascades. Among those that did, recommendations for dose reductions were often made without confirmation of a dose-dependent association, with most studies recommending the discontinuation of the index drug but not specifying an alternative medication. The persistence of potentially problematic drug combinations at hospital discharge identified in this study highlights the challenge physicians face in recognising and addressing prescribing cascades. It also points to the need for expert medication review at admission and particularly at discharge of older patients with multimorbidity and associated polypharmacy.
The identification and management of prescribing cascades are further complicated by the limitations of existing assessment tools. The ThinkCascades list, developed through three rounds of a modified Delphi validation process and involving international experts in geriatric pharmacotherapy, produced a list of only nine common and clinically important prescribing cascades [11]. This list very likely underrepresents the true number and prevalence of clinically relevant prescribing cascades. Although the Doherty list includes the 25 most commonly published appropriate and inappropriate prescribing cascades [7], some of the prescribing cascades listed raise questions about some of the cascades’ frequency and clinical relevance. Examples include lower urinary tract symptoms arising from statins leading to drugs for urinary frequency/incontinence and depression arising from direct oral anticoagulants (DOACs) leading to antidepressant drug prescription. These examples highlight the limitations of relying heavily on statistical methods such as PSSA to define cascades without clinical data, expert endorsement and clinical plausibility to validate proposed prescribing cascades. Nevertheless, a recent follow-up study evaluating the strength of the evidence supporting the prescribing cascades identified by Doherty et al. found that 84% of these prescribing cascades were supported by moderate evidence, i.e. single high-quality study or strong evidence, i.e. multiple high-quality studies [28].
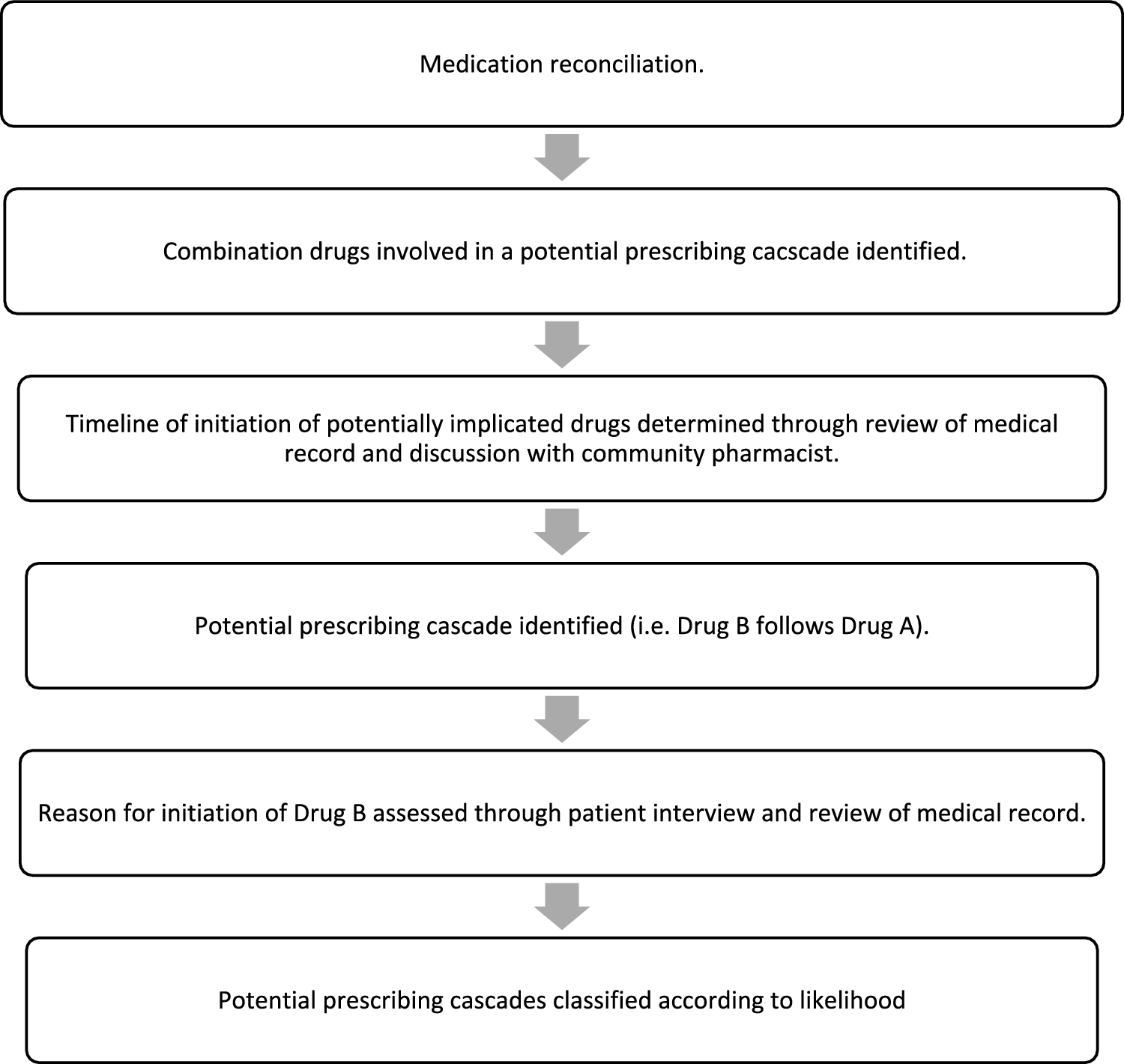
Most prescribing cascades in the present study were categorized as ‘possible’ or ‘uncertain’. Accurate identification of the prevalence of probable or definite prescribing cascades using the criteria applied in this study is likely to be challenging during medication review. Categorization of any clinical event as ‘probable’ or ‘certain’ in relation to multimorbid older patients requires rigorous assessment and therefore, as we have demonstrated, reliance on patient recall and physician or pharmacist documentation in patients’ medical records may not be sufficient. A prospective study design involving contemporaneous assessment of patients’ symptoms, as well as prescriber interviews, at the onset of possible prescribing cascades would be required for greater clarity. The feasibility of conducting such a labour-intensive study, likely with major recruitment challenges and resource implications, was beyond the scope of the present study.
A more comprehensive validated explicit list of clinically relevant prescribing cascades is likely required to enhance identification during routine medication review. In a recent commentary, O’Mahony and Rochon pointed out that the number of inappropriate prescribing cascades is potentially enormous but that more clinically relevant and common cascades can be identified more readily using a systems-based structured explicit cascades list approach that can be applied readily in a manner that is more suitable for routine medication review [29]. Such a structured, systems-based list of prescribing cascades could also be valuable as an educational tool in this important area of geriatric pharmacotherapy. Heightened awareness of potential cascades is likely to facilitate their prevention.
4.1 Study Limitations
This study has some limitations. First, the absence of a national electronic healthcare system in most public hospitals in Ireland, coupled with frequent transitions of care and missing medication initiation dates, made reconstruction of the chronology of potential prescribing challenging and at times wholly uncertain. This limited our ability to establish clear timelines between drug A and drug B initiation in some cases. However, there is no consensus in literature on the appropriate timeframe for defining prescribing cascades, which can range from a short number of weeks to several years. The timeframe can also vary according to the onset of ADE symptoms, which may vary between medications, as well as the recognition of ADEs which may depend on the timing of patients’ presentation to healthcare settings. For example, it may take many months to some years before antipsychotic medication leads to drug-induced parkinsonism leading to antiparkinsonian medication. In contrast, gastrointestinal upsets induced by acetylcholinesterase inhibitor therapy may lead to inappropriate proton pump inhibitor or antidiarrheal prescription within days. Second, as mentioned, patients’ medical records in the Irish public hospital system are still predominantly paper-based, with no widespread integrated electronic platform between community healthcare settings and hospital settings. This resulted in incomplete access to clinical data, particularly that relating to general practitioner assessments. Third, this study was conducted in a single hospital, which may limit the generalizability of the finding to other hospitals or healthcare settings. Finally, as this was an observational rather than an interventional study, we were unable to apply the definitive test for prescribing cascades, i.e. observation for resolution of ADE symptoms by discontinuing drug A.

Comments (0)