
Remember me
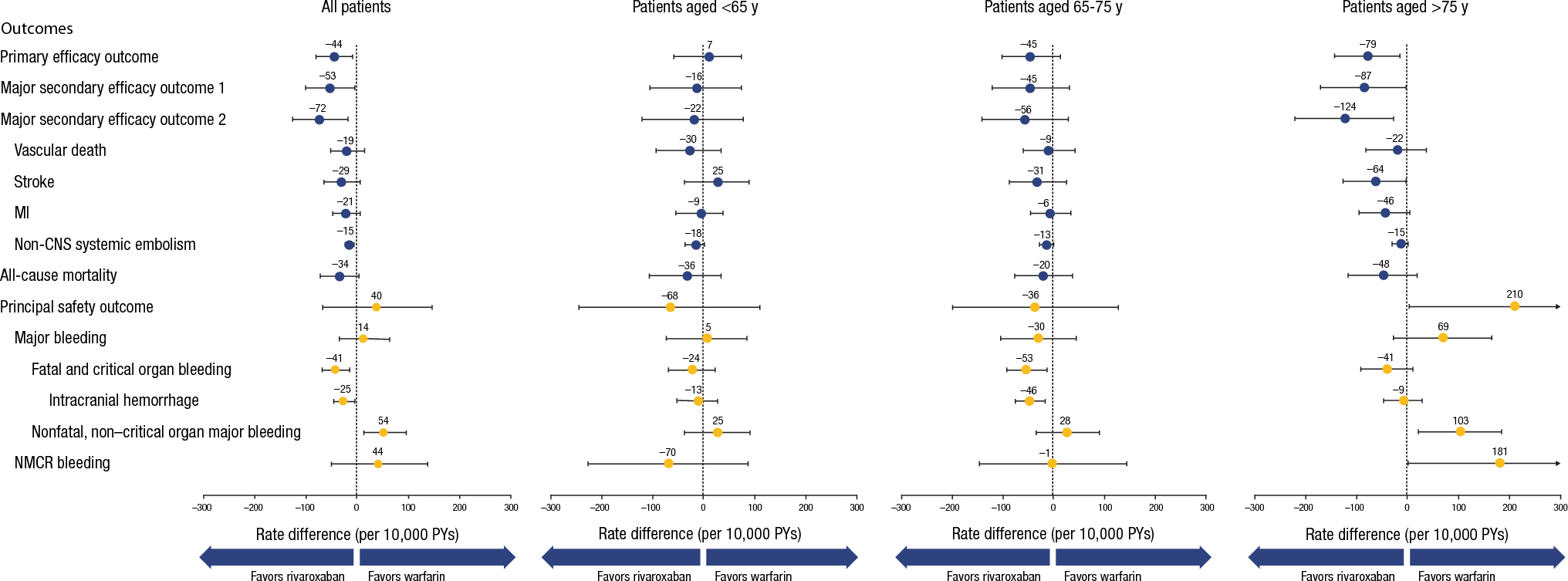
Of the 14,236 patients in the ROCKET-AF trial, 23% were < 65 years of age, 39% were 65–75 years of age, and 38% were > 75 years of age. The rate differences per 10,000 patient-years for different efficacy and safety outcomes are presented in Fig. 1 and Supplementary Online Resource Table 1. The rate difference (95% CI) for the primary efficacy outcome of stroke and systemic embolism (SSE) in the trial overall was −44 (−81, −8) events, favoring rivaroxaban over warfarin. The differences appeared to increase with age, with a rate difference of +7 (−59, 73) events for patients aged < 65 years, −45 (−102, 13) events for patients aged 65–75 years, and −79 (−143, −15) events for patients aged > 75 years. Most of this difference was driven by differences in stroke, with −29 (−65, 6) events favoring rivaroxaban in the overall trial and +25 (−39, 88) events, −31 (−88, 25) events, and −64 (−126, −2) events in the increasing age groups, respectively. For the composite endpoint of SSE, MI, and vascular death (major secondary efficacy endpoint 2), the rate difference in the overall study was −72 (−126, −18) events, favoring rivaroxaban over warfarin. As with the primary efficacy endpoint, the magnitude of the benefit of rivaroxaban increased with increasing age (−22 [−121, 77], −56 [−141, 29], and −124 [−221, −27] events in patients aged < 65, 65–75, and > 75 years, respectively). Note that for composite endpoints, patients are only counted once even if they have an event for each of the components.
Fig. 1
Rate differences (95% CI) per 10,000 PYs of rivaroxaban versus warfarin for efficacy and safety outcomes in patients with NVAF (ROCKET-AF, safety/on-treatment analysis set). CI confidence interval; CNS central nervous system; MI myocardial infarction; NMCR nonmajor clinically relevant; NVAF nonvalvular atrial fibrillation; PY patient-year. The primary efficacy outcome is the composite of stroke and non-CNS systemic embolism. The major secondary efficacy outcome 1 is the composite of stroke, non-CNS systemic embolism, and vascular death (includes deaths due to spontaneous bleeding, MI, stroke, heart failure, and arrhythmias). The major secondary efficacy outcome 2 is the composite of stroke, non-CNS systemic embolism, MI, and vascular death. The principal safety outcome is the composite of major bleeding and NMCR bleeding. Fatal bleeding requires that the death be adjudicated as vascular
In terms of safety, the rate difference (95% CI) in major bleeding in the trial overall was +14 (−35, 64) events, favoring warfarin over rivaroxaban (Fig. 1). The rate differences varied across the different age groups, with +5 (−74, 84) major bleeding events in patients aged < 65 years, −30 (−104, 45) events in patients aged 65–75 years, and +69 (−27, 166) events in those aged > 75 years. When considering the more clinically significant events of fatal bleeding and critical organ bleeding, the rate difference overall was −41 (−68, −15) events, favoring rivaroxaban. The rate differences were −24 (−70, 22) events in patients aged < 65 years, −53 (−92, −13) events in patients aged 65–75 years, and −41 (−92, 11) events in those aged > 75 years, with all groups favoring rivaroxaban.
When combining efficacy and safety events for an evaluation of NCB, events need to be of similar clinical impact to patients. Consequently, the NCB evaluation in these patients with NVAF was the combination of SSE, MI, vascular death, fatal bleeding, and critical organ bleeding. In the trial overall, the rate difference (95% CI) in the NCB was −84 (−142, −26) events, favoring rivaroxaban (Fig. 2 and Supplementary Online Resource Table 2). The rate difference grew from −25 (−128, 78) events in patients aged < 65 years, to −61 (−151, 30) events in patients aged 65–75 years, to −150 (−255, −45) events in patients aged > 75 years. Therefore, the NCB of rivaroxaban compared with warfarin in the ROCKET-AF trial is clearly favorable in older patients.
Fig. 2
NCB* incidence differences (95% CI) per 10,000 PYs (ROCKET-AF, safety/on-treatment analysis set) or per 10,000 patients (EINSTEIN DVT/PE and Extension, ITT analysis set; EINSTEIN CHOICE, full analysis set) for rivaroxaban versus comparators in patients with NVAF and VTE, overall and by age subgroups. CI confidence interval; CNS central nervous system; DVT deep vein thrombosis; ITT intention-to-treat; MI myocardial infarction; NCB net clinical benefit; NVAF nonvalvular atrial fibrillation; PE pulmonary embolism; PY patient-year; VTE venous thromboembolism. *NCB for NVAF (ROCKET-AF) is the composite of vascular death, stroke, MI, fatal bleeding, critical organ bleeding, and non-CNS systemic embolism; NCB for VTE (EINSTEIN studies) is the composite of symptomatic recurrent DVT, nonfatal or fatal PE, and major bleeding
Benefit–risk balance over time was also evaluated based on Kaplan–Meier cumulative incidence differences for the primary efficacy endpoint, major bleeding, and fatal/critical organ bleeding, as shown in Fig. 3 for patients aged ≥ 65 years and in Supplementary Online Resource Fig. 1 for the other age groups. Note that these plots reflect the between-treatment difference in rates, so while individual Kaplan–Meier cumulative incidences are monotonic, these curves can both increase and decrease over time. For patients aged ≥ 65 years, the primary efficacy endpoint and the composite of fatal and critical organ bleeding both favor rivaroxaban shortly after randomization and increasingly favor rivaroxaban over time. Major bleeding varies between no between-treatment difference and about 50 more events on rivaroxaban than warfarin per 10,000 patients. This shows benefits outweighing risks early and increasingly favoring rivaroxaban over time.
Fig. 3
Cumulative excess number of primary events versus major bleeding based on the Kaplan–Meier method, on treatment up to day 1140, in patients aged ≥ 65 years in the ROCKET-AF study (safety/on-treatment analysis set). On-treatment was the period between the date of the first double‐blind study medication to the date of the last double‐blind study medication administration plus 2 days. Efficacy and major bleeding were from randomization to first event; fatal (narrow definition) or critical organ bleeding was from first dose to first event. Negative values favor rivaroxaban, and positive values favor warfarin
3.2 Treatment of VTEOf the 8281 patients in the pooled EINSTEIN DVT and EINSTEIN PE trials, 63% were aged < 65 years, 23% were aged 65–75 years, and 15% were aged > 75 years. The difference (95% CI) in excess number of patients with an event per 10,000 patients based on Kaplan–Meier cumulative incidences at day 185 for the primary efficacy outcome of recurrent symptomatic DVT and nonfatal or fatal PE in the trial overall was −35 (−99, 29) events, favoring rivaroxaban (Fig. 4 and Supplementary Online Resource Table 3). The risk difference increased with age from −4 (−82, 74) events in patients aged < 65 years, to −40 (−170, 89) events in patients aged 65–75 years, and up to −164 (−359, 31) events in patients aged > 75 years.
Fig. 4
Risk differences (95% CI) per 10,000 patients based on Kaplan–Meier cumulative incidences at Day 185 with rivaroxaban versus enoxaparin/VKA for efficacy and safety outcomes in patients with VTE (pooled EINSTEIN DVT and EINSTEIN PE, ITT analysis set). DVT deep vein thrombosis; ITT intention-to-treat; NMCR nonmajor clinically relevant; PE pulmonary embolism; VKA vitamin K antagonist; VTE venous thromboembolism. The primary efficacy outcome is the composite of symptomatic recurrent DVT and nonfatal or fatal PE. The secondary efficacy outcome is the composite of symptomatic recurrent DVT, nonfatal or fatal PE, and all-cause mortality. The principal safety outcome is the composite of major bleeding and NMCR bleeding
Reflecting the reduction in major bleeding in the trial overall, the difference (95% CI) in excess number of patients with an event was −81 (−135, −27) events favoring rivaroxaban. The difference of in excess number of patients with major bleeding events improved for rivaroxaban in older patients, with +7 (−45, 59), −88 (−222, 47), and −436 (−641, −231) events in patients aged < 65, 65–75, and > 75 years, respectively. Interestingly, the risk difference grew in favor of rivaroxaban with each increased age category for every component of major bleeding (fatal bleeding, critical organ bleeding, need for transfusion of at least two units, and a drop in hemoglobin by at least 2 g/dL; Fig. 4). Consequently, the greatest difference in major bleeding with rivaroxaban occurred in the age groups most at risk for major bleeding.
In the EINSTEIN trials, NCB was defined as the combination of symptomatic recurrent DVT, nonfatal or fatal PE, and major bleeding (Fig. 2). In the trial overall, the risk difference (95% CI) in NCB was −103 (−185, −21) events, favoring rivaroxaban. The risk difference by age group was +3 (−90, 96) events in patients aged < 65 years, −105 (−287, 77) events in patients aged 65–75 years, and −544 (−815, −273) events in patients aged > 75 years. Therefore, the NCB of rivaroxaban compared with enoxaparin bridged to a vitamin K antagonist (VKA) in the pooled EINSTEIN DVT and EINSTEIN PE trials was clearly favorable in older patients and appears to be increasingly favorable with age.
Benefit–risk balance over time was also evaluated based on Kaplan–Meier cumulative incidence differences for the primary efficacy event and major bleeding, as shown in Fig. 5 for patients aged ≥ 65 years and Supplementary Online Resource Fig. 2 for the other age groups. Both the primary efficacy outcome and major bleeding start to favor rivaroxaban shortly after randomization and remain favorable for rivaroxaban throughout.
Fig. 5
Kaplan–Meier cumulative incidence difference of primary efficacy outcome events (symptomatic recurrent VTE) prevented and safety outcome events (ISTH major bleeding) caused, comparing rivaroxaban versus enoxaparin/VKA in patients aged ≥ 65 years (pooled EINSTEIN DVT and EINSTEIN PE, ITT analysis set). DVT deep vein thrombosis; ISTH International Society on Thrombosis and Haemostasis; ITT intention-to-treat; PE pulmonary embolism; VKA vitamin K antagonist, VTE venous thromboembolism. The x axis of the Kaplan–Meier figures is restricted to the period in which ≥ 10% of the analysis set subjects are at risk, as suggested by Pocock SJ, Clayton TC, Altman DG. Lancet. 2002;359:1686–1689
3.3 Secondary VTE PreventionThe role of rivaroxaban in longer-term secondary VTE prevention was first evaluated in the EINSTEIN Extension trial. Of the 1196 patients in the EINSTEIN Extension trial, 61% were aged < 65 years, 23% were aged 65–75 years, and 16% were aged > 75 years. In this trial, the risk difference (95% CI) per 10,000 patients for the primary outcome of symptomatic DVT and nonfatal or fatal PE was −604 (−828, −379) events, favoring rivaroxaban compared with placebo (Fig. 6 and Supplementary Online Resource Table 4). The risk differences were −549 (−824, −274), −556 (−1022, −90), and −837 (−1479, −196) in patients aged < 65, 65–75, and > 75 years, respectively.
Fig. 6
Risk differences (95% CI) per 10,000 patients based on Kaplan–Meier cumulative incidences at day 185 with rivaroxaban versus placebo for efficacy and safety outcomes in patients with extended VTE treatment (EINSTEIN Extension, ITT analysis set). DVT deep vein thrombosis; ITT intention-to-treat; NMCR nonmajor clinically relevant; PE pulmonary embolism; VTE venous thromboembolism. The primary efficacy outcome is the composite of symptomatic recurrent DVT and nonfatal or fatal PE. The secondary efficacy outcome is the composite of symptomatic recurrent DVT, nonfatal or fatal PE, and all-cause mortality. The principal safety outcome is major bleeding
The risk difference (95% CI) of major bleeding in the EINSTEIN Extension trial was +68 (2, 134) events, favoring placebo over rivaroxaban. The risk difference showed variation based on age group, with +57 (−22, 135) events, favoring placebo in patients aged < 65 years, and a zero difference in patients aged 65–75 years. The greatest risk difference was found in patients aged >75 years, with +236 (−88, 560) events, favoring placebo.
NCB in the EINSTEIN Extension trial included symptomatic DVT, nonfatal or fatal PE, and major bleeding (Fig. 2). The difference in NCB was −536 (−770, −301) events, favoring rivaroxaban. The risk difference (95% CI) favoring rivaroxaban increased in each of the age categories: −492 (−778, −207) events in patients aged < 65 years, −556 (−1022, −90) events in patients aged 65–75 years, and −601 (−1318, 115) events in patients aged > 75 years.
Benefit–risk balance over time was also evaluated based on Kaplan–Meier cumulative incidence differences for the primary efficacy outcome and major bleeding, as shown in Fig. 7 for patients aged ≥ 65 years. There is an increasing benefit favoring rivaroxaban through day 185 of treatment for the primary efficacy outcome; major bleeding reaches a plateau at day 98. A similar pattern is seen overall and in the 65–75 and > 75 years subgroups (Supplementary Online Resource Fig. 3).
Fig. 7
Kaplan–Meier cumulative incidence difference of primary efficacy outcome events (symptomatic recurrent VTE) prevented and safety outcome events (ISTH major bleeding) caused, comparing rivaroxaban versus placebo (EINSTEIN Extension, ITT analysis set) in patients aged ≥ 65 years. ISTH International Society on Thrombosis and Haemostasis; ITT intention-to-treat; VTE venous thromboembolism. The x axis of the Kaplan–Meier figures is restricted to the period in which ≥ 10% of the analysis set subjects are at risk, as suggested by Pocock S.J., Clayton T.C., Altman D.G. Lancet. 2002;359:1686–1689
In the EINSTEIN CHOICE trial, rivaroxaban 20 and 10 mg were compared with low-dose aspirin instead of placebo. Of the 3365 patients in the EINSTEIN CHOICE trial, 61% were aged < 65 years, 27% were aged 65–75 years, and 12% were aged > 75 years. The rate differences for the same primary efficacy endpoint as the other EINSTEIN trials were −312 events and −341 events favoring rivaroxaban 20 and 10 mg, respectively, compared with low-dose aspirin (Fig. 8). The rate difference for major bleeding in the trial overall did not favor rivaroxaban 20 mg (+28 events). There was a zero-rate difference between rivaroxaban 10 mg compared with low-dose aspirin in EINSTEIN CHOICE. Interestingly, the rate difference transitioned from favoring aspirin in patients aged < 65 years for rivaroxaban 20 mg (+72 events) and rivaroxaban 10 mg (+45 events), to favoring rivaroxaban in patients aged 65–75 years (−36 events for rivaroxaban 20 mg and −71 events for rivaroxaban 10 mg) and in those aged > 75 years (−71 for both rivaroxaban doses).
Fig. 8
Risk differences (95% CI) per 10,000 patients based on Kaplan–Meier cumulative incidences at 1 year with rivaroxaban versus aspirin for efficacy and safety outcomes in patients with extended VTE treatment (EINSTEIN CHOICE, full analysis set). The primary efficacy outcome is the composite of symptomatic recurrent nonfatal or fatal venous thromboembolism. The principal safety outcome is major bleeding
In the EINSTEIN CHOICE trial overall, the rate difference in NCB was −284 events favoring rivaroxaban 20 mg and −339 events favoring rivaroxaban 10 mg compared with low-dose aspirin (Fig. 2) [35]. The rate difference in NCB favored rivaroxaban 20 mg versus aspirin across all age subgroups at −255 events for patients aged < 65 years, −339 events for patients aged 65–75 years, and −338 events for patients aged > 75 years. Similarly, rate differences in NCB favored rivaroxaban 10 mg versus aspirin in all age subgroups with a smaller effect in patients aged > 75 years (−328 for patients aged < 65 years, −485 for patients aged 65–75 years, and −80 for patients aged > 75 years).
Using Kaplan–Meier cumulative incidence differences for the primary efficacy outcome and major bleeding, benefit–risk balance over time showed an increasing benefit favoring both doses of rivaroxaban compared with aspirin over 1 year for recurrent VTE for patients aged ≥ 65 years (Fig. 9). Similar patterns were observed overall and across all age subgroups for rivaroxaban 20 and 10 mg versus aspirin (Supplementary Online Resource Figs. 4 and 5).
Fig. 9
Kaplan–Meier cumulative incidence difference of primary efficacy outcome events (symptomatic recurrent VTE) prevented and safety outcome events (ISTH major bleeding) caused, comparing (A) rivaroxaban 20 mg and (B) rivaroxaban 10 mg versus aspirin (EINSTEIN CHOICE, full analysis set) in patients aged ≥ 65 years. ISTH International Society on Thrombosis and Haemostasis; VTE venous thromboembolism. The x axis of the Kaplan–Meier figures is restricted to the period in which ≥ 10% of the analysis set subjects are at risk, as suggested by Pocock S.J., Clayton T.C., Altman D.G. Lancet. 2002;359:1686–1689
Comments (0)