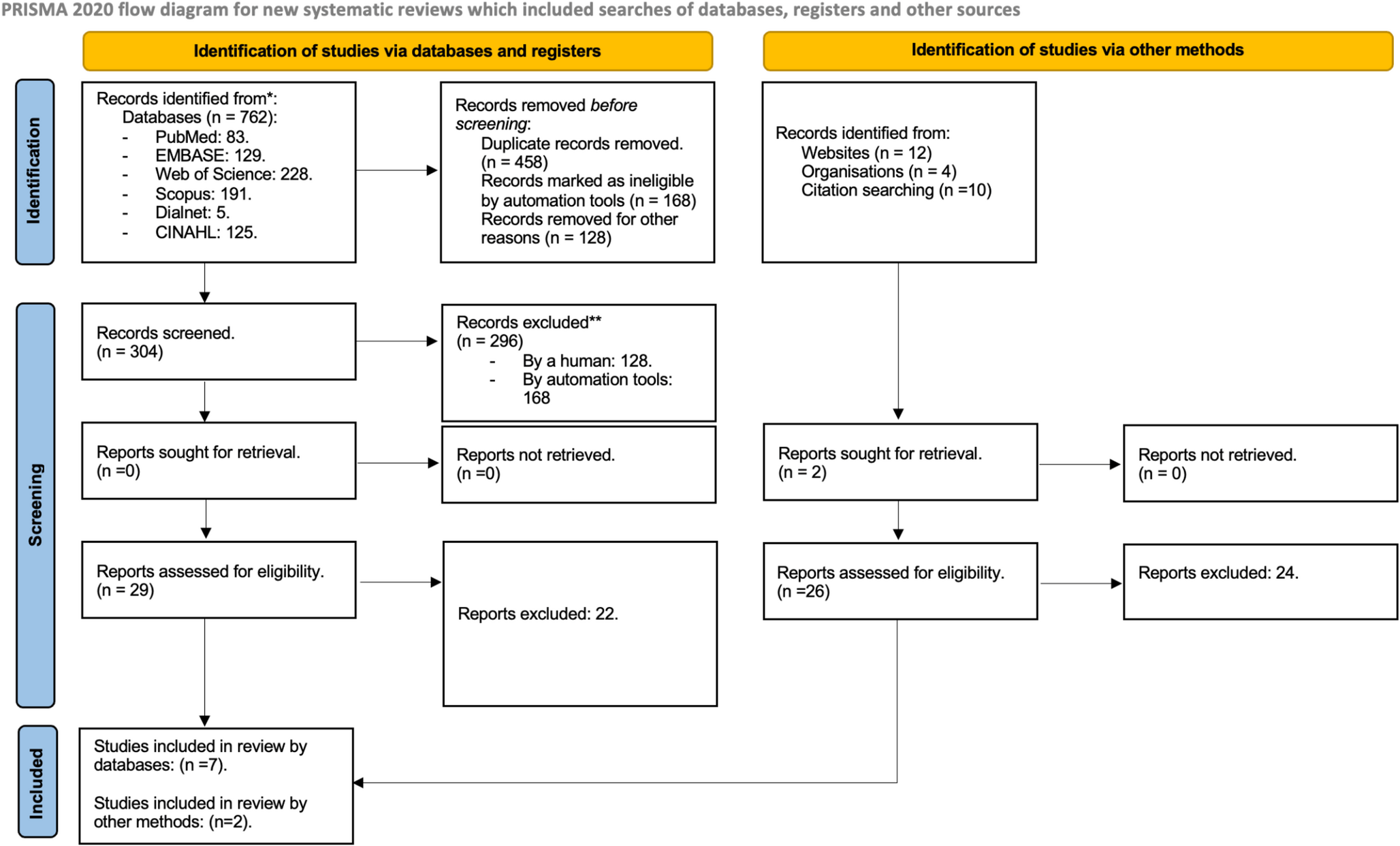
In this study, 74 cases of MA-associated deaths, investigated between 2005 and 2019 in Eastern Saxony, Germany, were evaluated. According to data published from Norway [21], this study is the first to address MA-related deaths in Europe.
Consistent with the majority of published papers on MA-associated deaths the deceased in Saxony were predominantly male (71.6%, Table 1). Interestingly, the deceased were significantly younger at the time of death (mean 29.59 years, Table 1) than in other studies [18, 27, 29]. No trend can be derived from the annual distribution of MA-related deaths in Saxony. The number of cases ranged from just one (2006, 2009) to twelve cases in 2015 (Table 1). Possibly, a significant number of MA-related deaths may remain unreported, contributing to a “dark field” of undetected fatalities [31].
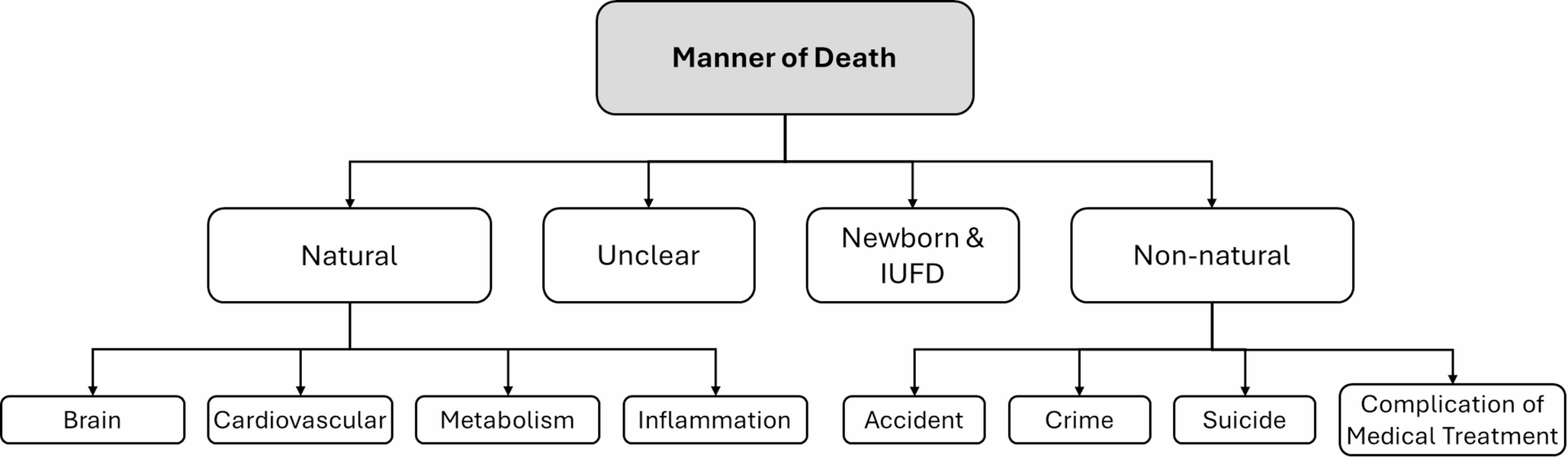
The largest group of non-natural methamphetamine (MA)-associated deaths in this study was the accident group, with intoxication being the primary cause of these accidents (Table 2). This finding is consistent with general literature on MA-related deaths [18, 27, 29, 32, 33]. Direct MA intoxication was the cause of death in 17.6% (n = 12) of all cases, including two cases with toxic MA blood concentrations and seven cases with comatose-lethal levels of MA. In the remaining cases, MA was present only as a toxicological finding, a pattern also observed in studies from Taiwan [33, 34], Japan [27], Iran [22] and Australia [18, 29, 32].
Suicides were the second most frequent cause of death following accidents (Table 2). The methods of suicide were predominantly violent, such as stab wounds to the body cavities, falls from height, and hanging, aligning with findings in the existing literature [18, 22, 27, 29, 32, 34]. Individuals with pathological consumption patterns of MA are at an elevated risk of suicide, particularly if they exhibit risk factors such as a Beck Depression Inventory score > 20 [35, 36], female gender, intravenous use, a history of severe depression, or previous inpatient treatment for psychiatric illness [18, 25, 29, 33, 34].
Criminal cases in the study involved victims of violent acts. The average MA blood concentration in these cases was in the lower range of MA exposure, supporting the theory that the victims were not the direct cause of their deaths due to MA but were rather victims of other violent acts. Notably, 75% (n = 3) of the intrauterine fetal demise (IUFD) observed in this cohort were categorized within this group.
The observation that significantly fewer natural deaths (Table 2) were recorded overall, and that the majority of natural deaths were due to cardiovascular causes (manifesting as LVH and increased heart weights), is consistent with findings in the literature [18, 22, 27, 29, 32, 33]. It is presumed that metabolic disorders and infections, common in chronic MA users, may have contributed to these natural deaths. These conditions include general neglect, poor management of chronic diseases like diabetes, intravenous drug abuse, and a weakened immune system, which predispose individuals to fatal conditions such as pneumonia, septic myocarditis, and encephalitis.
This study’s unique number of MA-associated deaths offers a more nuanced view of the relationship between MA intoxication and related fatalities. In contrast to the numerous studies on MA-related deaths, the present study also determined the MA blood concentration in the blood of the deceased. When compared to reference values starting at 0.20 µg/ml [37, 38] and toxic concentrations noted in the literature starting at ca. 0.50 µg/ml [18, 27, 37,38,39,40], the median lethal blood concentration measured in this study (8.65 µg/ml, Table 3) was ca. 17 times higher. During autopsy, all cases exhibited nonspecific signs of intoxication, including dilated hollow organs, liquid postmortem blood, pronounced brain and lung edema, acute congestion of parenchymal organs, and the presence of Tardieu spots. The median MA blood concentration in mixed intoxications (2.92 µg/ml, Table 3) was nearly six times higher than the toxic concentrations described in the literature [27, 37,38,39,40].
Darke et al. [18] and Stronach et al. [29] found that over approx. 40% of cases involved multiple substances, and this study similarly found that approx. 50% of cases had consumed both MA and at least one other drug. While Eastern Saxony exhibited fewer cases of poly-intoxication, the substances involved were similar to those reported internationally, including opiates, alcohol, antidepressants, and antipsychotic drugs [18, 22, 30, 32]. A direct comparison of autopsy material revealed that although the number of accidental drug intoxications was lower, MA intoxications were more prevalent in Eastern Saxony than in Australia [18, 29].
The results of this study, alongside comparable international research, highlight the urgent need for action to address MA use in Eastern Saxony. These findings reveal a pattern of precarious living conditions and social circumstances among the deceased, including high unemployment rates, singlehood, and low rates of parenthood. These factors may contribute to an elevated risk of MA-related fatalities [17, 24, 26, 33].
While MA still plays a relatively minor role in Germany overall, some countries worldwide are already severely affected. Individuals in socioeconomically precarious situations are especially vulnerable to MA-associated deaths [18, 22, 33]. To reduce this, preventive measures such as training programs aimed that professionals and the public can help raise awareness of the risks associated with MA use. Increased cooperation between law enforcement agencies, including the Federal Criminal Police Office and State Criminal Police Offices, is critical for combating the illegal drug trade and controlling the spread of MA, particularly in prisons. Furthermore, MA should be listed as a separate drug in official government datasets, rather than being grouped under stimulants or together with amphetamines in publications such as Police Crime Statistics. In addition, it appears essential that efforts be approached to reduce the “dark field” of unreported MA-related deaths.
Emergency medical personnel and rescue services play a crucial role in responding to MA-related incidents. Enhanced training for these professionals would enable them to recognize symptoms of MA intoxication more rapidly, improving their responses to acute emergencies and the accurate documentation of deaths [31]. Additionally, the implementation of specific ICD-10 coding for MA could aid in better tracking and reporting of MA-associated deaths. Currently, there is only one code (F15) for all stimulants, which complicates the recording of MA-related fatalities and hinders the development of targeted preventive measures.
In conclusion, as Stronach et al. formulated for Australia [29], there is also a need for screening and early management approaches in Germany. A first step could be an increased service level integration of mental health and drug treatment services. This study provides valuable insights into the impact of methamphetamine on public health in Eastern Saxony, Germany, and underlines the need for a comprehensive, coordinated approach to tackle the problem and reduce the number of deaths caused by MA.
Limitations
While this study provides valuable insights, there are several limitations to be considered, both within the context of this research and in comparison to other studies:
Geographic Limitations: The catchment area of this study is restricted to Eastern Saxony, which may limit the generalizability of the findings to other regions in Germany or internationally.
Sample Size: Although the case cohort is unique within Germany to date, it remains relatively small, which may impact the statistical power and the ability to draw broader conclusions.
Incomplete Sociodemographic Data: The dataset often lacks complete sociodemographic information, which could provide a more comprehensive understanding of the individuals involved and potentially identify additional risk factors or trends.
Unspecified Consumption Patterns: The form of methamphetamine consumption is frequently not specified in the data, which limits the ability.
to explore its role in the outcomes observed. There is a significant degree of heterogeneity in the methods of consumption, which complicates the analysis.
ICD-10 Coding Issues: The ICD-10 coding system, where all stimulants are grouped under the F15 code, does not differentiate between methamphetamine and other amphetamines. This can lead to misclassification in data reporting and make it difficult to track MA-specific fatalities in official records.
Postmortem Examination Limitations: Postmortem investigations are a significant limitation, as the “dark field” for drug-related and non-natural deaths is considerably larger than what is currently known or reported [31]. This means that the actual number of MA-associated deaths may be underreported, leading to potential underestimation of the problem.
These limitations should be taken into account when interpreting the results and when considering the broader implications for public health and policy.



Comments (0)