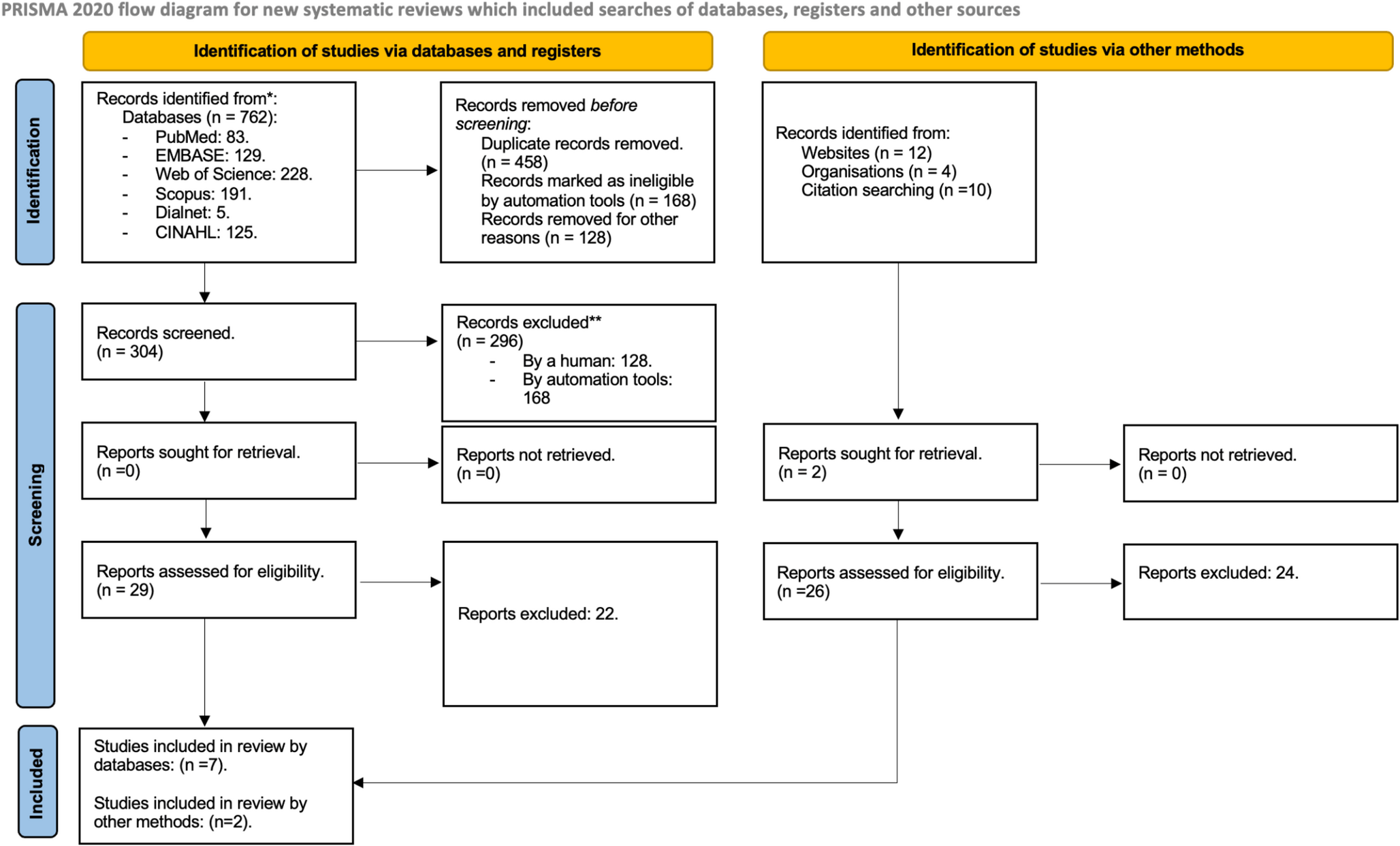
We identified 19 peer-reviewed articles reporting on subject injury rates and risk ratios after exposure to less-lethal force modalities during police interventions in real-life settings. Most articles retrieved data on UOF incidents from one source, as the article by Maguire that retrieved information from one source reporting on 2119 UOF incidents [25]. In contrast, three articles retrieved data from more than one source, such as the article by Jenkinson et al. retrieving information from 6 different sources [26]. Hence, information was based on information from a total of 26 sources (Table 2). In terms of context, most of the sources were from the US (n = 22), followed by the UK (n = 3) and Canada (n = 1). Subjects exposed to police less-lethal UOF were predominantly men (75.8-94%) (Table 2). Data spanned from 1998 to 2020; however, four articles did not report on year of observation [26,27,28,29]. Regarding data sources, 22 sources concerned CEW, 15 concerned physical force, 14 concerned OC spray, 10 concerned canine, and 9 concerned baton (Table 2). Four articles contained information on models of CEW: “pre-M26-weaponry”, M26 and X26 [24, 26, 30, 31] (Table 2). A few articles used composite grouping of force modalities: Less-lethal weapons (OC spray, pepper ball launchers, CEWs, rifles and shotguns using less-lethal shells, and riot shields), other physical methods (various forms of physical force, impact weapons such as batons, canines, and the forcible stop of a fleeing vehicle), and impact weapons (batons, flashlights, tear gas, and rubber bullets) [32, 33].
Table 2 Descriptive statistics, including author(s), years of data, number of data, civilian male sex, types of use of force modality and quality assessment scoreInjuries following exposure to UOF were largely based on data on UOF incidents from registers kept by law enforcement agencies (e.g., UOF forms). Additionally, two studies collected data on injuries as a result of UOF from national surveillance system databases (e.g., Centers for Disease Control and Prevention (CDC)) or data from a CEW manufacturer (e.g., Taser International) [26, 34, 35]. However, the definition of a UOF incident was not clear in every study; for example, whether an incident was characterized by a police intervention or by the number of force methods in a police intervention. A UOF incident might also include multiple officers or subjects, or multiple modalities. Only two articles presented sufficient data on UOF incidents (police encounters with a subject), subjects, and the total amount of force utilized (number of applied force modalities) [24, 36]. The number of UOF incidents reported in the included articles ranged from 467 to 34,217, resulting in 117,789 incidents (Table 2). Besides reporting on UOF incidents, data presentation was based on the number of CEW deployments, the number of patients treated at hospitals, or the number of observed injuries owing to police UOF (Table 2) [26, 34, 35, 37].
As data were based on law enforcement registries, injuries were often defined and registered by police personnel who were obliged to fill out UOF forms. However, two articles allowed physicians to review the data from police agencies together with medical records, classifying the injuries according to severity (mild, moderate, or severe) [24, 38]. Two articles reported using trained coders to read police reports and code content [35, 39]. Another approach was to create an injury severity index in categories of subjects voicing an injury, visible injuries as noted by police, transportation to hospital, subjects in need of medical attention, or subjects hospitalized [29, 33, 37, 40]. Two articles clearly stated that puncture wounds from probes of a CEW were not defined as an injury [41, 42], while this was not apparent in the other articles. Five articles reported on specific injuries/diagnoses following exposure to force modalities [26, 30, 35, 38, 39]. With reference to our quality assessment, 9 articles were deemed high quality (A), while the remaining 10 scored low quality (B) (Table 2).
The rate of subject injury following exposure to CEW ranged from 0 to 75.6% (Table 3a). The weighted mean injury rate across all articles reporting on subject injury following CEW was 24.5%. The rate was similar across the high-quality articles (26.8%) (Table 3b). Subject injury following OC spray ranged from 2.3 to 74.5% (Table 3a). The weighted mean of subject injury for all articles and high-quality articles exclusively were 20.2% and 6%, respectively (Table 3b). The rates of injury to subjects exposed to baton, canine, and physical force ranged from 3.8 to 80%, 4–100%, and 11–78%, respectively (Table 3a). The corresponding weighted mean injury rates for all and high-quality articles were 30.4% and 40.7% following the use of baton, 43.4% and 95.7% following the use of canines, and 59.4% and 31.4% following the use of physical force (Table 3b). In comparison to the weighted mean injury rate, the mean injury rate for the use of baton and canine across all articles were higher (44.8% and 62%, respectively). The rate of subject injury following the composite group impact weapons (batons, flashlights, tear gas, and rubber bullets) was 74% (Table 3a).
Table 3a Subject injury rates following different use of force modalities as reported in the included studiesTable 3b Mean and weighted mean subject injury rates of all and quality A articles (standard deviation in parenthesis)In terms of risk ratios for subject injury following exposure to less-lethal force modalities, three out of four articles indicated a decrease of subject injury following CEW by 65–87% compared to all other uses of force [30, 41, 42] (Table 4a). However, when compared specifically to physical force and OC spray, CEW increased the likelihood of subject injury [29]. In contrast, physical force was generally associated with an increase in risk of injuries compared to all other uses of less-lethal force, except for one study [25, 30, 39, 41]. The use of canines as a force modality increased the likelihood of subject injury regardless of reference category (all other use of force, CEW, and physical force) [24, 25, 30, 33]. In turn, OC spray reduced the risk of subject injury by 69–92% in comparison to all other types of force and 81% compared to CEW specifically [30, 33, 41, 42]. The composite group less-lethal weapons including OC spray, pepper ball launchers, CEW, rifles and shotguns using less lethal shells, and riot shields reduced subject injury by 51% in comparison to the composite group other physical methods including various forms of physical force, impact weapons such as batons, canines, and the forcible stop of a fleeing vehicle [32] (Table 4a).
Table 4a Risk ratios of subject injury following different use of force modalitiesTable 4b Risk ratios of subject injuries following implementation of CEW in agenciesFour articles reported on risk ratios of subject injury before and after implementation of CEW, alternatively in comparison with agencies not using CEW as a force modality (Table 4b). Three out of four studies reported a 30–78% reduction of subject injury after introduction of CEW [26, 37, 41]. However, after the implementation of CEW in several US custodies higher death rates among prisoners were observed [28].
Specific injuries following CEW were often mild such as superficial puncture wounds from probes or blunt trauma following falls (contusions, lacerations, superficial burn marks, fractures of finger and nasal bones). Moderate or severe injuries were rare and included head injuries such as temporoparietal intraparenchymal contusion and cerebellar epidural hematoma, or rhabdomyolysis [38]. Two subjects having been in an intensive struggle with the police collapsed unexpectedly 20 and 5 min, respectively, after exposure to CEW. Both subjects died. At autopsy one subject had dilated cardiomyopathy, and cocaine present in the blood, the other subject had antipsychotic drugs present in the blood. In both cases, no information on cause of death was given. However, the medical examiner determined that CEW was not a contributing factor [38]. Other injuries following CEW were internal injuries (not further specified) or teeth fractures [35, 39]. The specific injuries observed following physical force were bone fractures, traumatic brain injuries, and hemopneumothorax [24]. In addition, one cardiac arrest in association with physical force was reported; however, a causal association between death and UOF exposure was not established [24]. Finally, injuries associated with canines include bites to the extremities, bruises, and fractures [24, 26]. Such injuries were also seen following OC spray and the use of baton [26].
Regarding conflict of interest or funding, eight articles clearly stated that there were no competing interests [24, 25, 31, 34, 35, 38, 39, 42], four articles had a biography on authors in which there appeared to be no conflict of interest [29, 36, 37, 41]. In six articles there was no clear statement of competing interest, nor did the biography of authors allow for transparency [27, 28, 30, 32, 33, 40]. In one article one of the authors had undertaken a literature review paid for by a CEW manufacturer [26].



Comments (0)