
Remember me


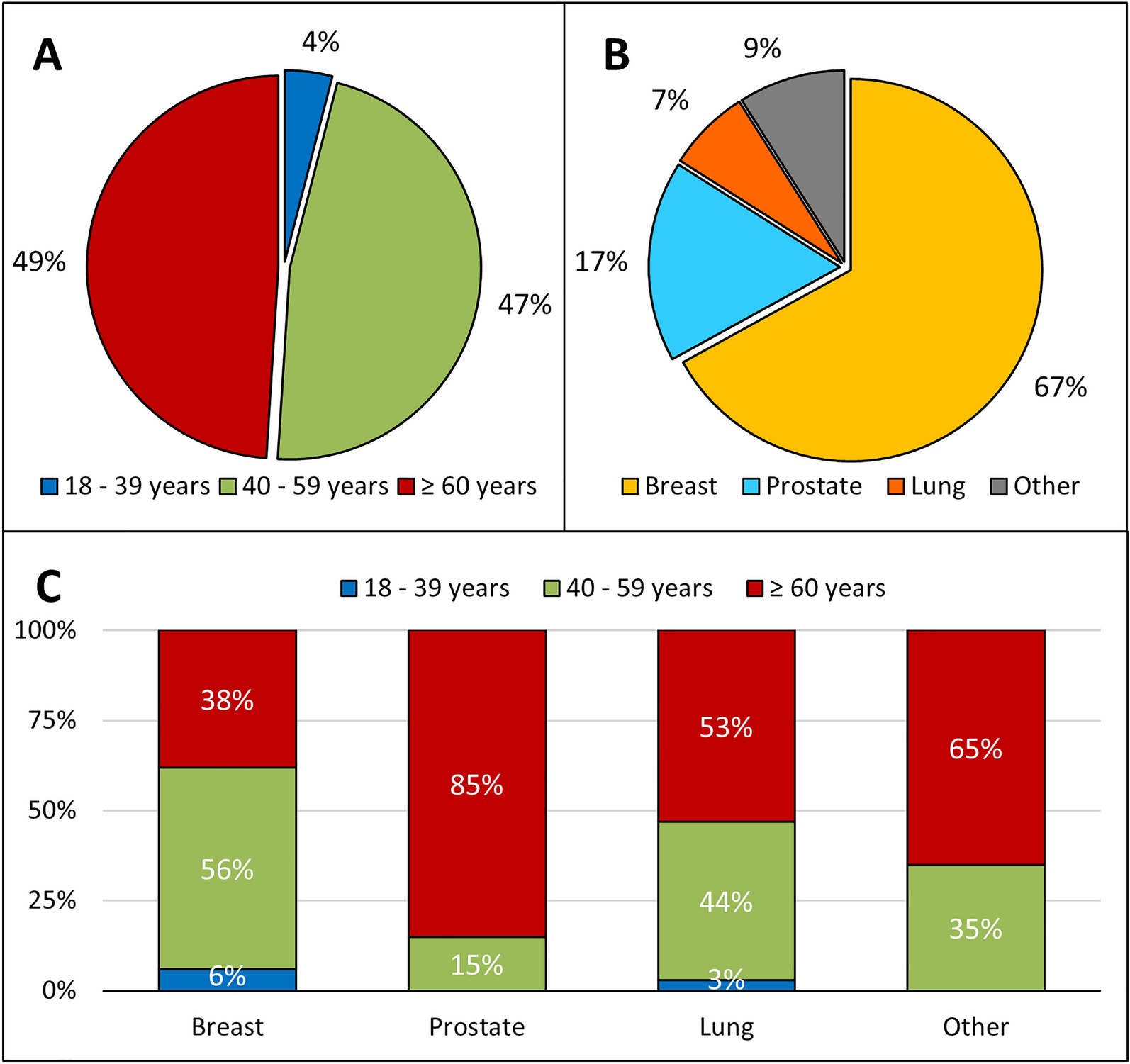

In total, 199 patients who met eligibility criteria were included in the study (mean age 59.1 years, 64.3% [n = 128] male, 35.7% female [n = 71], 72.9% white ethnicity [n = 145], 1.5% Asian ethnicity [n = 3], 0.5% Black ethnicity [n = 1] and 25.1% unknown ethnicity [n = 50]). Of these, 162 (81.4%) patients were being treated for a/mMM, and 37 (18.6%) were being treated for aRCC (Table 1). Median follow-up from index was 14.5 months (IQR: 7.2–26.2). In patients with a/mMM, metastases were present in 99.4% (n = 161), with lung and lymph node being the most frequent sites (53.7% [n = 87] and 52.5% [n = 85], respectively). The majority of patients had an Eastern Cooperative Oncology Group (ECOG) performance score of either 0 (58.6%, n = 95) or 1 (40.1%, n = 65), received ICI therapy as first-line treatment (63.6%, n = 103) and were initiated on NIVO + IPI (78.4%, n = 127). NIVO monotherapy or IPI monotherapy were received by 11.1% (n = 18) and 10.5% (n = 17) of patients, respectively. In patients with aRCC, metastases were present in 91.9% (n = 34) of patients, and the lung was the most frequent site (55.9%, n = 19). The largest proportion of patients had an ECOG performance score of 1 (59.5%, n = 22), and received ICI therapy as either first-line treatment (43.2%, n = 16) or second-line treatment (35.1%, n = 13). In total, 54.1% (n = 20) of patients with aRCC received NIVO monotherapy, while the remaining 45.9% (n = 17) received NIVO + IPI.
Table 1 Patient demographics and baseline clinical characteristicsIncidence and Grade of First irAEsAmong patients with a/mMM, 75.3% (n = 122) reported an irAE, with 45.9% (n = 56) of these patients reporting a grade 3 or 4 irAE (Table 2). When stratified by ICI therapy received, irAEs were reported by 77.8% (n = 14) of patients receiving NIVO monotherapy, 47.1% (n = 8) receiving IPI monotherapy and 78.7% (n = 100) receiving NIVO + IPI. Grade 3/4 irAEs were reported by 5.6% (n = 1), 11.8% (n = 2) and 41.7% (n = 53) of patients receiving NIVO monotherapy, IPI monotherapy or NIVO + IPI, respectively. More than one irAE was reported by 38.9% (n = 7) of patients receiving NIVO monotherapy, 17.6% (n = 3) receiving IPI monotherapy and 59.8% (n = 76) receiving NIVO + IPI during the study period. When further stratified by irAE type, colitis/diarrhoea and skin reactions were the most frequently reported irAE types across all ICI therapy groups: NIVO monotherapy (44.4% [n = 8] and 22.2% [n = 4], respectively), IPI monotherapy (35.3% [n = 6] and 17.6% [n = 3], respectively) and NIVO + IPI (42.5% [n = 54] and 37.8% [n = 48], respectively; Fig. 1a). Across all patients with a/mMM, independent of treatment received, colitis/diarrhoea, skin reactions, endocrinopathies, rheumatological and neurological toxicities and pneumonitis irAEs were more commonly classified as grade 1/2, whereas nephritis/renal dysfunction was more commonly classified as grade 3/4 (Supplementary Material Online Resource Table S1).
Table 2 irAE incidence and gradingFig. 1
Incidence of irAEs based on the most frequently reported (≥ 3%) irAE types within the a a/mMM and b aRCC cohorts. Data are stratified by ICI treatment and reported as a proportion of patients in that ICI treatment group. Counts correspond to the number of patients experiencing an irAE in that ICI treatment group. a/mMM advanced (unresectable or metastatic) malignant melanoma, aRCC advanced renal cell carcinoma, ICI immune checkpoint inhibitor, irAE immune-related adverse event
A total of 62.2% (n = 23) of patients with aRCC reported an irAE; 30.4% (n = 7) of those reported were grade 3/4. When stratified by ICI therapy received, irAEs were reported by 60.0% (n = 12) of patients receiving NIVO monotherapy and 64.7% (n = 11) of patients receiving NIVO + IPI, with grade 3/4 irAEs reported by 15.0% (n = 3) and 23.5% (n = 4) of patients receiving NIVO monotherapy or NIVO + IPI, respectively. More than one irAE was reported by 35.0% (n = 7) of patients receiving NIVO monotherapy and 35.3% (n = 6) receiving NIVO + IPI. When further stratified by irAE type, patients receiving NIVO monotherapy most frequently reported skin reactions (20.0%, n = 4), and those receiving NIVO + IPI most frequently reported skin reactions and hepatitis, with both reporting 35.3% (n = 6; Fig. 1b). In patients with aRCC, independent of treatment received, all irAEs were more commonly graded as 1/2 than as grade 3/4 (Supplementary Material Online Resource Table S1).
Median Time to First irAE OnsetIn patients with a/mMM, the median time to first irAE onset was 4.9 weeks (IQR: 2.9–9.4; Table 2). Median time to onset for grade 3/4 irAEs was 7.7 weeks (IQR: 3.4–13.1). When stratified by ICI therapy received, median time to onset was 12.6 weeks (IQR: 5.4–25.4) for patients receiving NIVO monotherapy, 4.2 weeks (IQR: 2.8–7.5) for those receiving IPI monotherapy and 4.6 weeks (IQR: 2.8–9.1) for those receiving NIVO + IPI. When further stratified by irAE type, the shortest median time to irAE onset was reported for skin reactions across all ICI therapy groups: NIVO monotherapy (3.1 weeks [IQR: 2.5–10.6]), IPI monotherapy (3.0 weeks [IQR: 1.8–3.9]) and NIVO + IPI (3.1 weeks [IQR: 2.1–10.1]; Fig. 2a). The median time to onset of first irAEs stratified by irAE type is presented in Supplementary Material Online Resource Table S2.
Fig. 2
Median time to first irAE onset based on the most frequently reported (≥ 3%) irAE types within the a a/mMM and b aRCC cohorts. Data are stratified by ICI treatment group. a/mMM advanced (unresectable or metastatic) malignant melanoma, aRCC advanced renal cell carcinoma, ICI immune checkpoint inhibitor, irAEs immune-related adverse events
Among patients with aRCC, median time to first irAE onset was 4.9 weeks (IQR: 2.9–9.4), and 7.7 weeks (IQR: 3.4–13.9) for grade 3/4 irAEs. When stratified by ICI therapy received, median time to onset was 13.5 weeks (IQR: 7.9–37.7) for patients receiving NIVO monotherapy, and 3.7 weeks (IQR: 3.0–15.2) for those receiving NIVO + IPI. The irAE type with the shortest reported median time to onset was colitis/diarrhoea for those receiving NIVO monotherapy (7.0 weeks [IQR 4.6–26.7]) and rheumatological toxicity for those receiving NIVO + IPI (0.1 weeks [IQR 0.1–0.1]; Fig. 2b). Median time to onset stratified by irAE type is presented in Supplementary Material Online Resource Table S3.
Management of First irAEsAmong patients with a/mMM reporting irAEs (n = 122), immunomodulating drugs were prescribed to 69.7% (n = 85) of patients, with the largest proportion of these patients receiving corticosteroids alone (81.2%, n = 69; Table 3). Of those patients who developed a grade 3/4 irAE (n = 56), 62.5% (n = 35) were prescribed corticosteroids alone, and 26.7% (n = 15) were prescribed one or more additional immunomodulating drug, including methotrexate (n = 1), mycophenolate (n = 9), tacrolimus (n = 1) or the tumour necrosis factor (TNF) inhibitor infliximab (n = 7). When stratified by the type of irAE reported, patients reporting hepatitis were most frequently prescribed immunomodulating drugs (75.0%, n = 33). The proportion of patients who were prescribed immunomodulating drugs stratified by the type of irAE reported is presented in Supplementary Material Online Resource Table S4.
Table 3 Use of immunomodulating drugs for irAE managementOf those patients with aRCC reporting any irAE (n = 23), 56.5% (n = 13) were prescribed immunomodulating drugs for irAE management, with 92.3% (n = 12) of these patients receiving corticosteroids alone. Of those patients who developed a grade 3/4 irAE (n = 7), 57.1% (n = 4) were prescribed corticosteroids alone. Data stratified by irAE type is presented in Supplementary Material Online Resource Table S5.
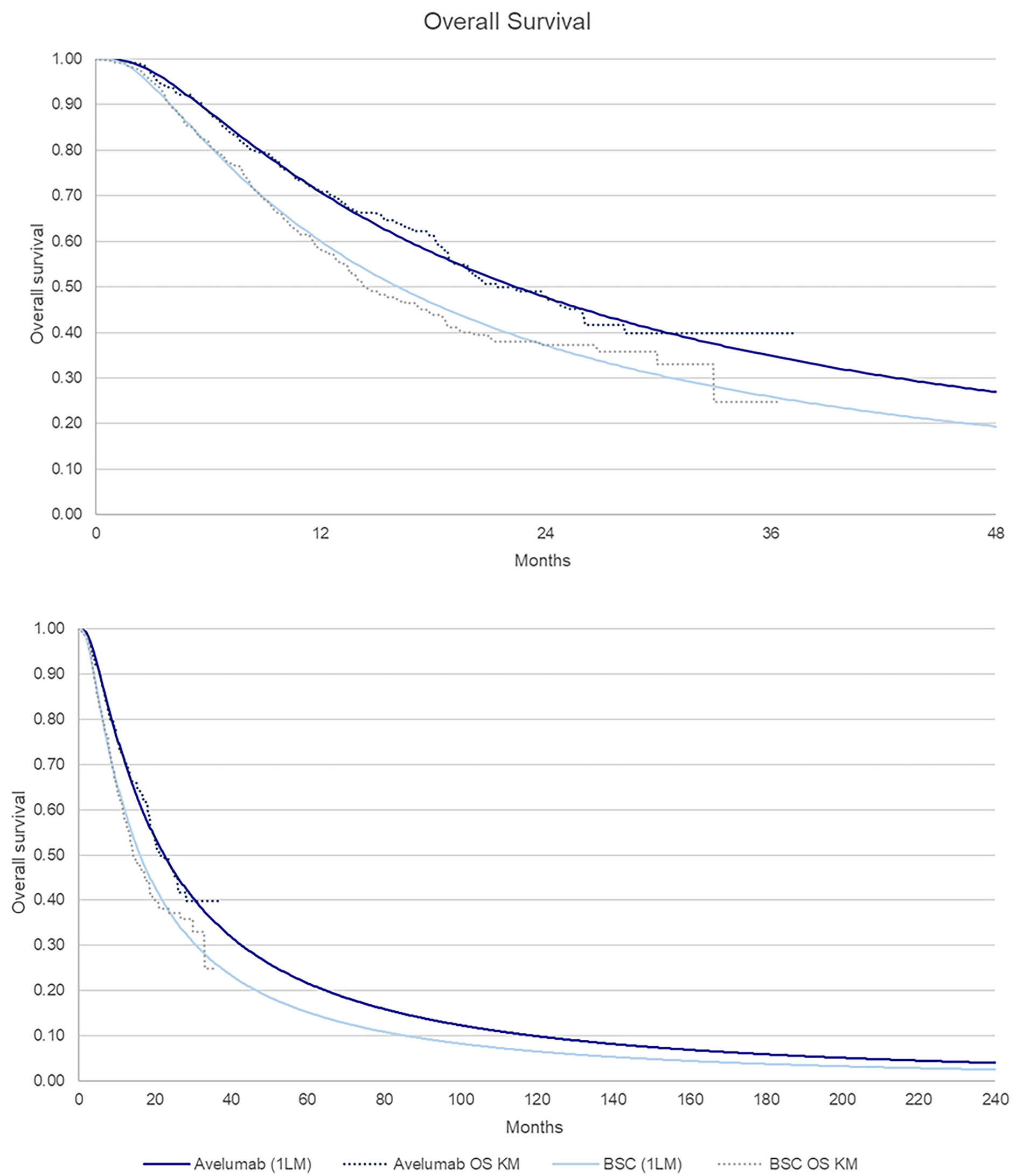
Overall SurvivalIn both the a/mMM and aRCC cohorts, median OS was numerically longer for patients who had experienced an irAE compared with those who did not (Fig. 3). In the a/mMM cohort, the median OS for patients who reported any irAE was 31.1 months (95% confidence interval [CI]: 20.3, not reached), with 12-, 24- and 36-month OS probabilities of 71.4%, 57.5% and 46.2%, respectively (Fig. 3a). For those patients who did not report an irAE, median OS was 14.8 months (95% CI: 10.6, not reached), with 12-, 24- and 36-month OS probabilities of 54.4%, 41.1% and 37.4%, respectively. Median OS in patients who experienced a grade 3/4 irAE was similar to that observed in patients who experienced a grade 1/2 irAE at 39.4 months (95% CI: 20.3, not reached) and 35.6 months (95% CI: 20.0, not reached), respectively (Supplementary Material Online Resource Fig. 1a).
Fig. 3
Overall survival stratified by whether an irAE was or was not reported by patients in the a a/mMM and b aRCC cohorts. a/mMM advanced (unresectable or metastatic) malignant melanoma, aRCC advanced renal cell carcinoma, CI confidence interval, irAE immune-related adverse event, NR not reached
In the aRCC cohort, median OS for any reported irAE was 38.4 months (95% CI: 19.1, not reached), with 12-, 24- and 36-month OS probabilities of 80.5%, 56.3% and 56.3%, respectively (Fig. 3b). Where no irAE was reported, median OS was 10.7 months (95% CI: 9.1, not reached), with 12- and 24-month OS probabilities of 49.1% and 24.6%, respectively. Median OS in patients who experienced a grade 1/2 irAE was 38.4 months (95% CI 19.1, not reached) whereas median OS was not reached in patients who experienced a grade 3/4 irAE (Supplementary Material Online Resource Fig. 1b).
Comments (0)